Case Report
A Rare Case of Isolated Proximal Interruption of the Right Pulmonary Artery
Naukarkar V*, Varma R and Shetty D
Department of Radio diagnosis, Nair Hospital, Mumbai, India
*Corresponding author: Naukarkar V, Department of Radio diagnosis, Nair Hospital, Mumbai, India, Phone: +91
8767207597; E-mail: naukarkarvikrant@gmail.com
Copyright: © 2023 Naukarkar V, et al. This is an open access article distributed under the Creative Commons Attribution
License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is
properly cited.
Article Information: Submission: 02/02/2023; Accepted: 10/03/2023; Published: 15/03/2023
Abstract
Proximal interruption of the pulmonary artery (PIPA) is a rare congenital anomaly. Presentation varies from mild breathlessness to life-threatening
hemoptysis. In isolation, this anomaly has a very good prognosis. But when associated with cardiac abnormalities the prognosis depends on the associated
conditions. Therefore, accurate and prompt diagnosis is very essential. Here we describe a case of proximal interruption of the pulmonary artery presenting
with mild hemoptysis which was managed conservatively.
Keywords
Pulmonary Artery Anomalies; Interrupted; Radiology; Case Report
Introduction
Proximal interruption of the pulmonary artery is an abnormality
where a proximal portion of a pulmonary artery shows abnormal
development with preserved, normally developed intrapulmonary
vasculature. It creates a condition of chronic hypoxia which leads
to a lot of physiological alterations. Here, we describe an interesting
case, where PIPA led to collateral vessel formation, the rupture of
which caused the patient to present with mild hemoptysis which was
managed conservatively.
Case Presentation
A 31-year-old male presented to the casualty department with
complaints of acute onset on-and-off fever, mild hemoptysis,
vomiting, abdominal pain, and loose stools. On probing further,
he also gave a history of mild chronic dyspnea on exertion. The
patient was mildly hypotensive with tachypnoea and tachycardia
but maintained oxygen saturation. He denied any addictions.There
was no history of any surgery in the past. A respiratory examination
revealed reduced respiratory sounds on the right side of the chest. Cardiovascular, neurological, and abdominal examinations were
normal.
Routine investigations were ordered as per the hospital
protocol. Electrocardiographic findings were within normal limits.
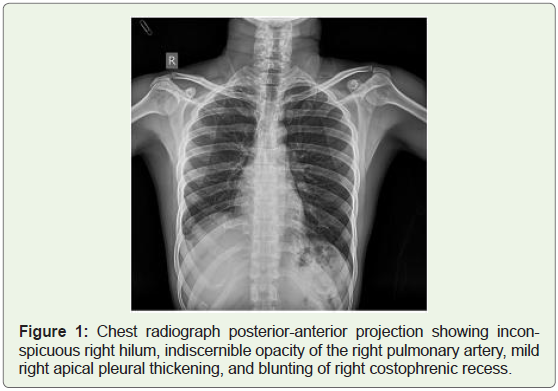
Hematological cell counts were adequate. Chest X-ray revealed mild
elevation of the right dome of the diaphragm and apical pleural
thickening. Mild blunting of the right costophrenic recess was noted.
Bony thorax and heart size were appropriate. What was surprising to
us was the inconspicuous right hilum and indiscernible opacity of the
right pulmonary artery (Figure 1). It was decided to go ahead with
computed tomography pulmonary angiography with high-resolution
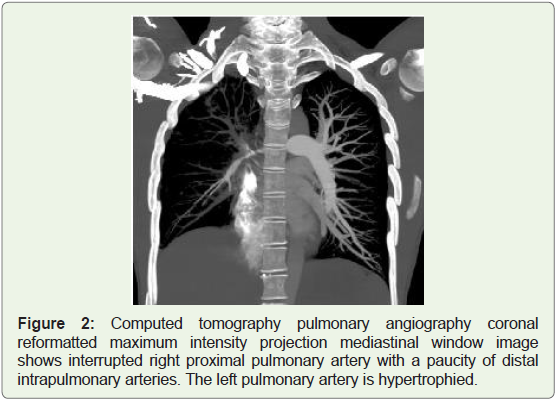
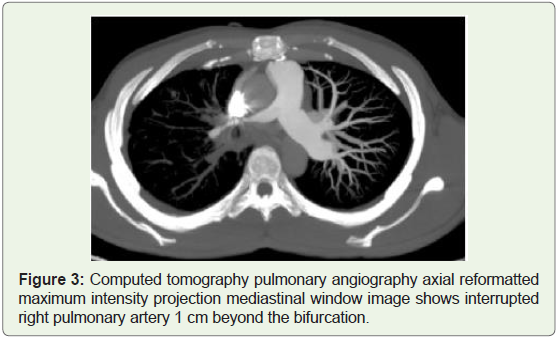
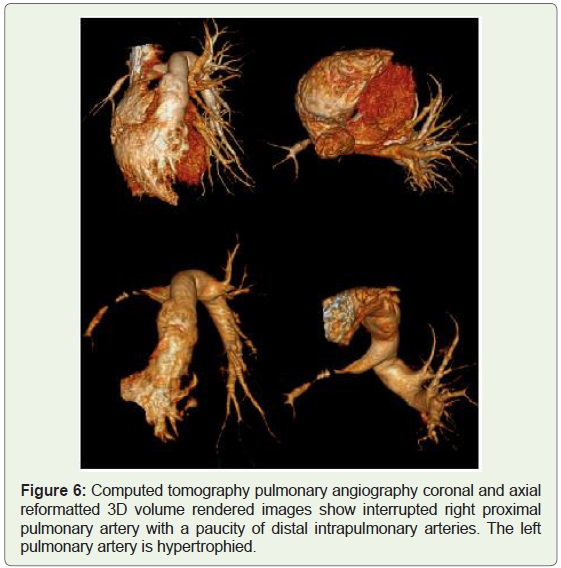
thoracic sections. CT revealed the right proximal pulmonary artery
interruption after 1 cm of origin. The left pulmonary artery was
hypertrophied (Figure 2). There was a paucity of peripheral pulmonary
vasculature which appeared narrow in caliber as compared to the
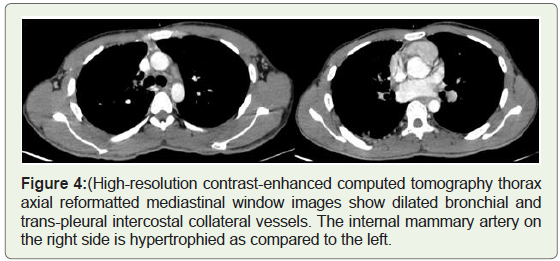
left side. Multiple enlarged bronchial, Trans plural collateral vessels
were observed supplying right lung parenchyma. The right internal
mammary artery was larger in caliber than the left. Mild pleural
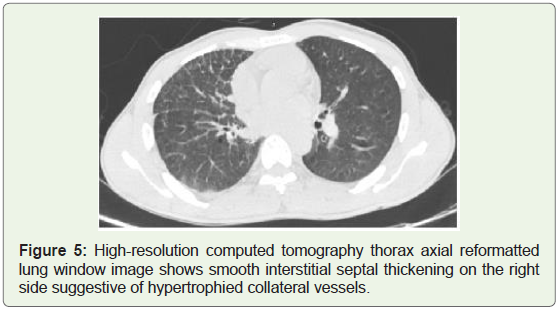
thickening was noted. The lung window revealed right-sided smooth interstitial septal thickening suggestive of hypertrophied collateral
vessels. The tracheobronchial tree revealed no abnormalities.
Due to the recent Leptospira outbreak in the rainy season, the
patient was evaluated with anti-leptospiral antibodies which came
positive. Because of mild symptomatology, it was decided to treat
the patient conservatively. The patient was started on ceftriaxone and
adequate hydration was maintained to tackle hypotensive status. The
patient improved dramatically within a week. For interrupted rightsided
pulmonary artery follow-up was suggested as the patient only
had associated mild chronic dyspnea on exertion (Figure 3).
Discussion
Proximal interruption of the right pulmonary artery (PIPA) is
a rare congenital anomaly with a reported prevalence of 1:2,00,000.
Usually, PIPA occurs on the side opposite to that of the aortic
arch. It is more common on the right side. When on the left side it
is associated with cardiac anomalies and a right-sided aortic arch.
The most common cardiac anomalies are tetralogy of Fallot, patent
ductus arteriosus, and atrioventricular septal defects. Left-sided
anomaly presents earlier and at a young age. Proximal pulmonary
arteries develop from the proximal 6th aortic arch in the first trimester
of pregnancy. The distal part of the left 6th aortic arch forms ductus arteriosus while the distal part is involuted on the right side. PIPA
develops from abnormal development of the proximal part of the
6th aortic arch. Intrapulmonary vasculature has a separate origin
and hence is developed normally. Three groups of the anomaly are
recognized. In group 1 there is the presence of a left to right shunt
most commonly patent ductus arteriosus. In group 2 associated
pulmonary hypertension is present. An isolated anomaly without
associated pulmonary hypertension is seen in group 3 [1].
Patients with PIPA are mostly asymptomatic or present with mild
symptoms. The most common symptoms include chronic exertional
dyspnoea, decreased exercise tolerance, recurrent infections, and
hemoptysis. Reduced blood flow and hypoplasia of the lung lead to
progressive dyspnoea on exertion. Recurrent respiratory infections
are caused by the decreased delivery of systemic immunomodulators
due to the interruption of blood supply proximally. Rupture of
hypertrophied thin-walled collateral vessels can cause hemoptysis [2].
Diagnosis of the abnormality can be suspected on chest
radiography based on findings of absent pulmonary artery opacity,
and inconspicuous hilum. Other associated findings include
ipsilateral lung volume loss with ipsilateral cardio mediastinal shift
and elevation of the hemidiaphragm. Compensatory hyperinflation
of the contra lateral lung with herniation to the opposite side can
be seen. Collateral vessel formation leads to peripheral reticular
opacities, pleural thickening, and rib notching. Recurrent infection
can cause cystic-bronchiectasis changes.
Computed tomography pulmonary angiography (CTPA) is
widely done to diagnose PIPA since it is rapid, readily available, and
hasan excellent spatial resolution (Figure 4). Collateral vessels are
better appreciated. Thin 0.625 mm sections are obtained from lung
apices to the top of the diaphragm after giving 1.5 ml/kg contrast at
the rate of 3.5-4 ml/sec bolus dose. Maximum intensity projection
reformats are made. A high-resolution lung window better assesses the
bronchial tree and lung parenchyma. Normally developed bronchial
tree is seen. CT findings include proximal interruption of the
pulmonary artery with preserved or paucity of the distal pulmonary
vasculature. Lung parenchyma is perfused by systemic hypertrophied
collateral vessels from bronchial, trans-pleural intercostal, internal
mammary, phrenic, subclavian, and brachiocephalic arteries. These
changes can lead toperipheral reticulations, pleural thickening, and
rib notching. Sometimes an aberrant artery arising from the aorta can be seen supplying the lung parenchyma. Ipsilateral volume loss
of lung parenchyma with mediastinal shift, crowding of ribs, and
elevation of the hemidiaphragm is seen. Compensatory contra lateral
lung volume expansion and hypertrophy of the pulmonary artery are
noted. Intraparenchymal and subpleural cysts and bronchiectasis
changes can be seen in cases of recurrent infections.
Magnetic resonance angiography (MRA) of the thorax is an
alternative to a CT scan. Respiratory and electrocardiographic
gating is used to acquire better images. T1 and T2 weighted TSE
images in axial and coronal planes are obtained in minimum free
breathing or breath holding as per the patient’s condition. Pre- and
post-gadolinium contrast images with subtraction are also acquired.
However, due to limited availability, long duration, and cost
consideration CT is preferred over MRI. The only indication of MRI
is in young patients to avoid radiation exposure (Figure 5).
Digital subtraction angiography best depicts proximal
interruption of the pulmonary artery and offers simultaneous
intervention in cases of hemoptysis.
Other investigations include a ventilation-perfusion scan (V/Q
scan). It shows decreased perfusion on the side of interruption with
maintained ventilation. Echocardiography can be done to look for
associated cardiac anomalies [3].
PIPA is managed conservatively depending on the
symptomatology. Rarely in case of severe symptoms intervention is
needed. Recurrent infections are treated with appropriate antibiotics.
Chronic breathlessness due to pulmonary hypertension seen in 19-
27% of patients requires treatment with phosphodiesterase inhibitors
and endothelin receptor antagonists. Hemoptysis is seen in 10-20
% of cases. It is self-limiting most of the time. When significant, percutaneous trans-arterial embolization of bleeding collateral
vessels is done. Various embolization materials include gel foam,
polyvinyl alcohol, glue, and coils. It carries a success rate of 73-99 %
and a recurrence rate of 10-55 %. In cases of recurrent hemoptysis
even after embolization, pneumonectomy is performed. Surgical
reconstruction of interrupted pulmonary artery can be done but the
procedure carries high morbidity and mortality [4] (Figure 6).
Hypogenetic lung syndrome is one of the differentials where
hypoplasia of lung parenchyma with anomalous venous drainage
is seen. A scimitar-shaped abnormal draining vein along the right
heart border differentiates this condition from PIPA. Swayer James
syndrome can mimic PIPA where unilateral lung hypoplasia with
increased lucency will be seen due to post-infectious obliterative
bronchiolitis. Unlike PIPA air trapping will be seen on expiratory
images. Primary pulmonary hypoplasia is characterized by the
hypoplasia of normal lung parenchyma, bronchial tree, and
pulmonary vasculature. On the contrary in PIPA bronchial tree is
normal. Pulmonary artery branch stenosis is one of the differentials
but can be ruled out by the absence of post-stenotic dilatation [5].
Conclusion
Proximal interruption of the pulmonary artery is an uncommon
congenital anomaly with varied presentation. Due to the benign nature
of the disease, it needs to be differentiated from other more ominous
conditions by appropriate investigations. PIPA is mostly managed
conservatively unless complicated by significant hemoptysis, where
in percutaneous transarterial embolization or pneumonectomy is
performed.
References
Citation
Naukarkar V, Varma R, Shetty D. A Rare Case of Isolated Proximal Interruption of the Right Pulmonary Artery. Indian J Appl Radiol. 2023;9(1): 179.