Research Article
Anatomical Variations of Pulmonary Venous Drainage among Indian Population
Shah A*, Joshi A and Yash Achhapalia
Department of Radio-diagnosis, Lokmanya Tilak Municipal Medical College and General Hospital, Sion, Mumbai, India
*Corresponding author: Shah A, Department of Radio-diagnosis, Lokmanya Tilak Municipal Medical College and General
Hospital, Sion, Mumbai, India; mobile: +91 9969120898; E-mail: ankitasrad@gmail.com
Copyright: © 2022 Shah A, et al. This is an open access article distributed under the Creative Commons Attribution License,
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article Information: Submission: 15/08/2022; Accepted: 09/09/2022; Published: 16/09/2022
Abstract
Background: The drainage sites of the pulmonary veins are an important source of ectopic atrial electrical activity, especially in patients with atrial
fibrillation. Variations in the pulmonary venous anatomy are frequent. Differences in pulmonary vein anatomy and the presence of variant or anomalous
anatomy can be of critical importance, especially for preoperative planning of pulmonary and cardiac surgery.
Objective: To assess the patterns of pulmonary venous drainage into the left atrium and to determine the frequency of each variant of pulmonary venous
anatomy
Materials and methods: 300 studies of thoracic multidetector computed tomography were retrospectively reviewed for the anatomical features of the
pulmonary vein and its drainage pattern into the left atrium. The percentage of each pattern was calculated.
Results: The anatomy of pulmonary venous drainage in 300 patients (163 male and 133 female, mean age 45 years) showed some variation. In the
right pulmonary vein, the most common drainage pattern was two ostia (77.33%), followed by three to four ostia (19%) and a single ostium (3.67%). On the
left side, there were three patterns; a single venous ostium (63.33%) was much more common than two ostia (35.67%). Three ostia were seen in 3 cases
(1%). In both right and left pulmonary veins, there were six cases that had a single pulmonary venous ostium, bilaterally.
Conclusion: Variations in PV anatomy are not uncommon. Although frequently asymptomatic, knowledge of these variations is important in while
planning cardiothoracic surgeries and PV isolation..
Keywords
CT; Pulmonary veins; Variations
Introduction
The vascular system of the human body shows a plethora of
different patterns in every individual. This is known as normal
variation. Although the function of the pulmonary veins as a conduit
for oxygenated blood is clear, they carry special importance for
radiologists with regard to their anatomy and physiologic function.
The pulmonary venous drainage site is an important source of
ectopic atrial electrical activity, frequently initiating paroxysms
of atrial fibrillation [1]. Increasingly, selective radiofrequency
ablation of these arrhythmogenic foci is performed to treat patients
with refractory atrial fibrillation. The invasive procedures very
heavily depend upon the precision of mapping atrial anatomy [2].
Differences in pulmonary vein anatomy and the presence of variant
or anomalous anatomy can be of critical importance, especially for
preoperative planning of pulmonary and cardiac surgery. Knowledge
of pulmonary and cardiac vasculature forms a vital part of thoracic
interventions, not only for diagnostic purposes but also to predict and
prevent perhaps life threatening complications.
Objective
To assess the patterns of pulmonary venous drainage into the left
atrium and to determine the frequency of each variant of pulmonary
venous anatomy.
Materials & Methods
Study population:
Following institutional ethics committee approval, 300 studies of
thoracic multidetector computed tomography in between May 2021
to August 2021 performed for various indications were retrospectively
reviewed. Anatomical features of the pulmonary vein and its drainage
pattern into the left atrium was observed. The percentage of each
pattern and combination of patterns was calculated.Inclusion and Exclusion criteria:
All thoracic computed tomography scans of patients above the age
of 15 were included. Cases in which images showed poor pulmonary
vein enhancement, distorted anatomy of either the pulmonary
veins or lung parenchyma by mediastinal or lung pathologies were
excluded.CT data set:
All CT examinations were obtained by Philips Brilliance 64 slice
CT or Toshiba Aquilon Prime 160 slice CT with patient in the supine
position and holding a deep breath. The data for each case was taken
by one of the four major scans: 1) Contrast-enhanced conventional
CT chest, 2) CT pulmonary angiography, 3) CT aortogram and 4) CT
coronary angiogram. The scans were acquired with 0.9 mm thickness.
Soft copy DICOM images were retrieved from TeraRecon Aquarius
workstation (San Mateo, Calif).Pulmonary vein classification and statistical analysis:
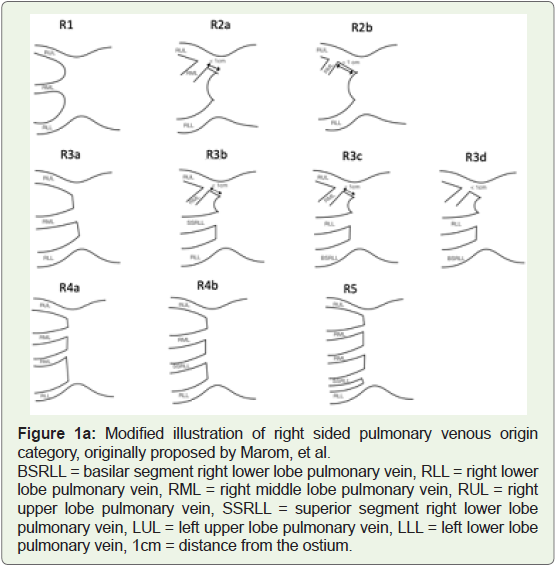
Marom EM et al. classified the pulmonary vein and its drainage
orifices into 6 patterns on the right side and 2 patterns on the left side
[3].Results
A total of 163 male and 133 female patient scans were studied
with ages ranging from 15 to 94 and a mean age of 45. Using Marom’s
pulmonary venous drainage categories, the drainage patterns were
summarized in Table 1 for the left pulmonary vein and Table 2 for the
right pulmonary vein with L3 in table 1 and R3d in table 2 proposed
as a new addition to the original classification by Marom (Figure 1A and B).
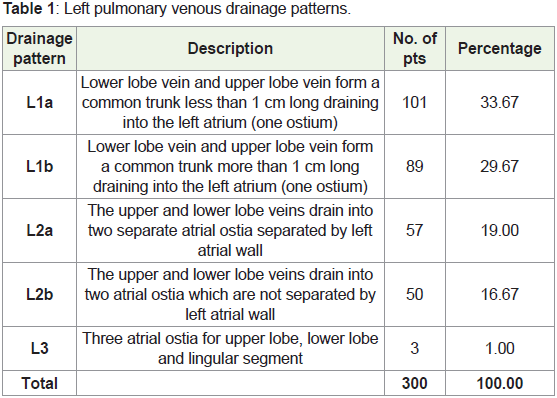
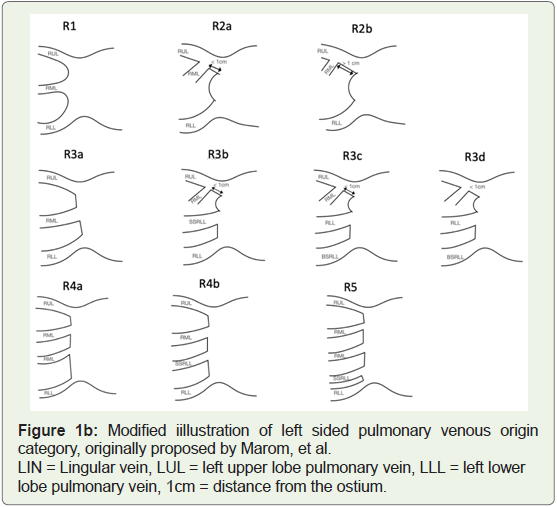
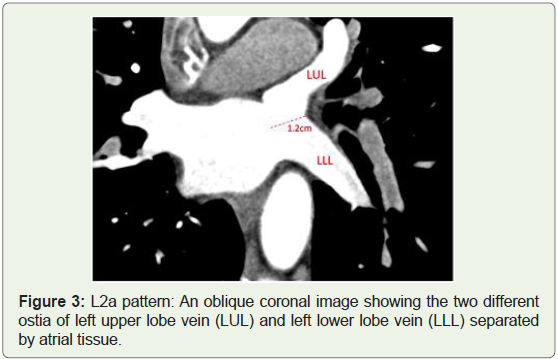
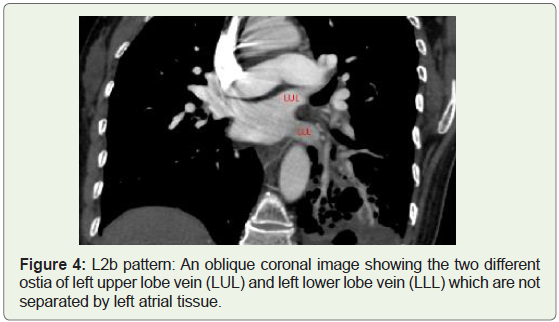
Left pulmonary venous drainage patterns (Table 1): There were
107 (35.66%) patients with two ostia for the upper and lower lobe
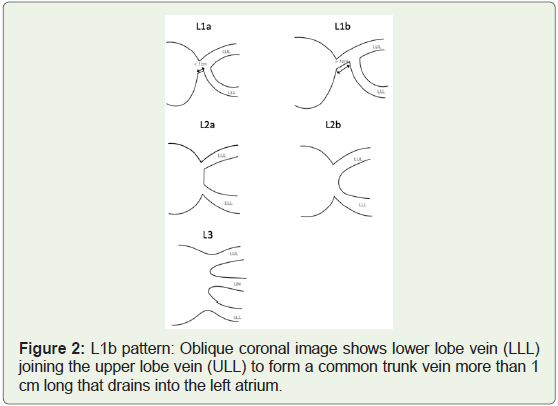
veins. A common trunk forming one ostium in the left atrium was
seen in 190 (63.33%) patients, which was a slightly higher percentage
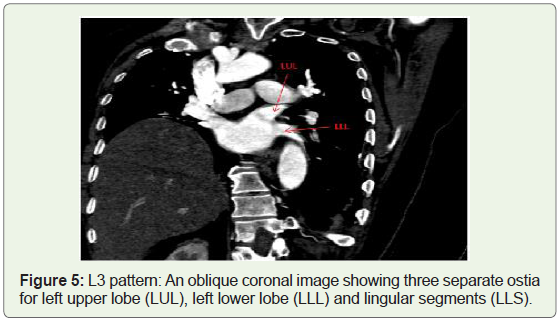
than the patients with two ostia. 1 cases (1%) differed from the
original Maroms classification in having three ostia for upper lobe,
lower lobe and linguilar segment. We propose a new category for this
variation as L3. (Figures 2-5).
Right pulmonary venous drainage patterns (Table 2): Most
patients (232, 77.33%) had the expected anatomy of two atrial ostia
for upper and lower lobe veins, with the middle lobe vein joining
the upper lobe vein. 11 cases (3.67%) had a single common ostium
opening into the left atrium. 5 cases (1.67%) had 4 ostia opening
into the left atrium for the upper, middle, superior segment, and
lower lobe veins. 52 cases (17.33%) had 3 ostia opening into the left
atrium for upper and middle lobe veins and a variable vein. Out of
these 52 cases, 5 cases have anatomy which differed from the original
Maroms classification having three atrial ostia for the lower, lateral segment of middle and upper lobe veins, with upper lobe veins being
accompanied by medial segment of middle lobe vein forming a
common channel. We propose a new category here as R3d in which
we found three atrial ostia for the lower, lateral segment of middle
and upper lobe veins, with upper lobe veins being accompanied by
medial segment of middle lobe vein forming a common channel
(Figures 6-9).
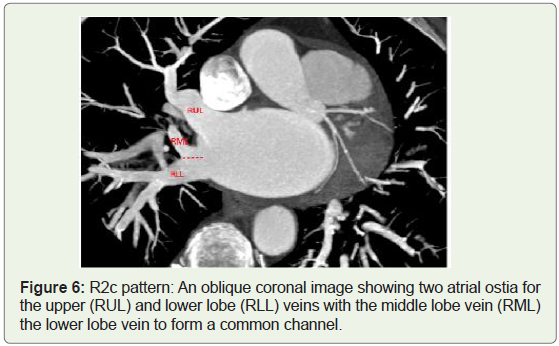
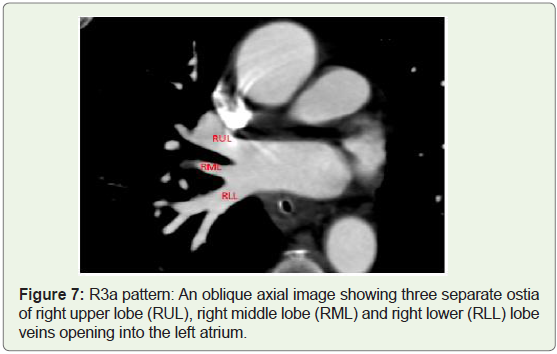
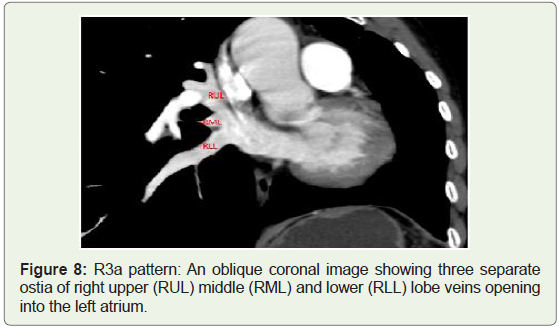
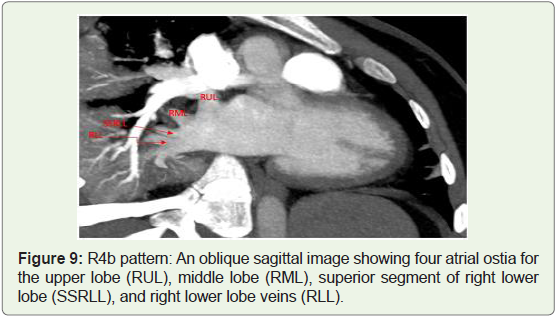
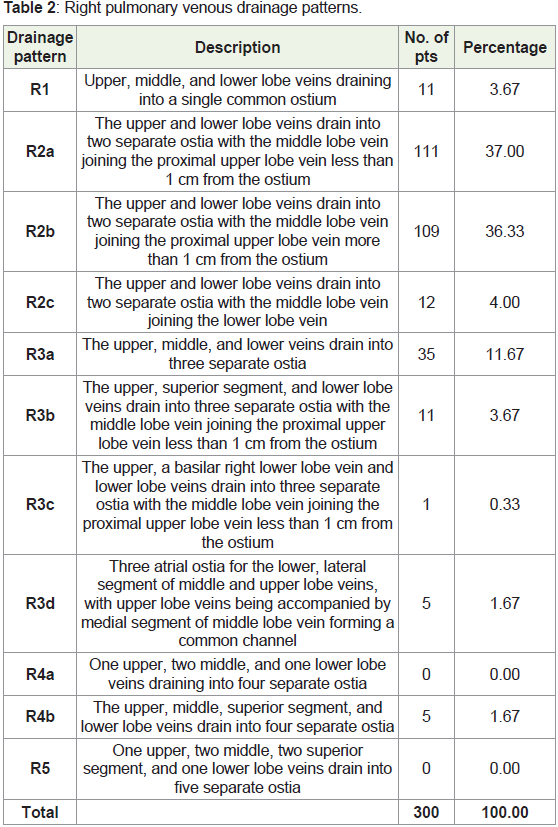
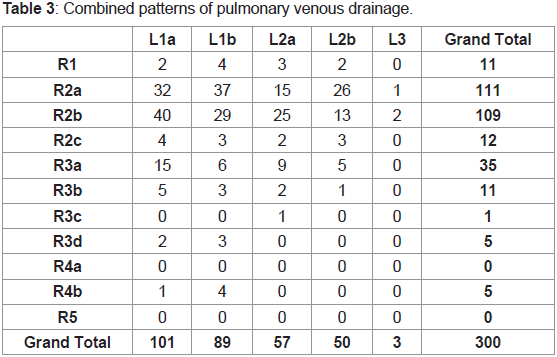
Table 3 discusses permutations and combinations of all the
categories of left sided and right sided drainage. Majority cases
(145, 48.33%) had two ostia draining from the right side and one
common ostium draining from the left side, with the most common
combination being R2b with L1a having 40 cases (13.33%) followed
by R2a with L1b with 37 cases (12.33%).
Discussion
Embryology and Development:
Around 4th week of intrauterine development, a primitive
common pulmonary vein originates from a greater splanchnic
capillary network that extends from the heart to the liver and connects
to the cardinal and umbilicovitelline veins [4,5]. A small strand arises
from this network to connect with the left atrium which makes its
connection and forms a venous lumen, a sleeve of myocardial tissue
envelops the new vein from the surrounding mesenchymal tissues
[6]. This primitive pulmonary vein connects the lung bud’s venous
network to the left atrium close to the atrioventricular junction. Along
with the development of the primary atrial septum on their right side
the final positions of the pulmonary vein orifices are determined in the
morphologic left atrium. The left atrium drains the tributaries of the
primitive pulmonary vein as they develop and along with the atrophy
of the connections to the cardinal and umbilicovitelline systems,
which forms separate pulmonary and systemic venous systems.Anatomy:
Pulmonary venous anatomy shows variations in the number
and the arrangement of drainage pattern and because of this fact
[3,7], It is best to consider pulmonary vein arrangement in terms of
commonality. In most people (57%-82%), four separate and distinct
pulmonary vein ostia arise from the left atrium [8,9]. Two of these ostia
are on the right, draining the right superior pulmonary vein and the
right inferior pulmonary vein; and two ostia are on the left, draining
the left superior and inferior pulmonary veins. Commonly, left atrial
tissue separates these ostia on the right but is not separated from each
other on the left. It can be tedious to delineate a common ostium
from separate ostium without connecting atrial tissue. However,
extrapolating the shape of the left atrium as it nears the pulmonary
vein ostia provides help with the same, to determine the expected
location of the pulmonary venoatrial junction [10,11]. Along with
different ostial patterns, numerous branching and drainage patterns
have been identified, with several investigators attempting to group
and categorize the patterns [12]. The most accepted classification
system for pulmonary venous drainage was produced by Marom et
al [3].Radiological Approach for Pulmonary Vein Evaluation:
CT and MR imaging, both depict the pulmonary venous anatomy well. However, CT offers a speed advantage, compared with MR
imaging which has greater spatial resolution. Electrocardiographically
gated cardiac CT should be ideally used for a detailed assessment of
pulmonary veins. For identification of the pulmonary venous number
and branching patterns, multiplanar reformatted images should be
preferred.Conclusion
At chest imaging, the pulmonary veins are an often overlooked
part of the anatomy that can become directly or indirectly involved
in a wide array of pathological and non pathological processes.
Detailed knowledge of the pulmonary veins is a necessity, because
imaging can play a critical role in differentiating normal findings
from serious conditions involving the pulmonary veins and hence
having vital application in multiple areas of cardiothoracic surgery
and interventional cardiology.
References
Citation
Shah A, Joshi A, Yash A. Anatomical Variations of Pulmonary Venous Drainage among Indian Population. Indian J Appl Radiol. 2022;8(1): 174.