Case Report
Subungual Glomus Tumour of Right Ring Finger; MRI Features
Kumar MK*, Priyadharshini V and Varma RR
Department of Radio-diagnosis, SRM Medical college hospital & Research Centre, Irungalur, Trichy-621105
*Corresponding author: Kumar MK, Department of Radio-diagnosis, SRM Medical college hospital & Research Centre,
Irungalur, Trichy-621105; E-mail: drmkrishnakumar@gmail.com
Copyright: © 2021 Kumar MK, et al. This is an open access article distributed under the Creative Commons Attribution
License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is
properly cited.
Article Information: Submission: 03/09/2021; Accepted: 08/12/2021; Published: 11/12/2021
Abstract
Glomus tumors are benign vascular neoplasms rarely found on the hand especially in the subungual region. Glomus tumors usually appear as a
reddish-green or pink nail plate with an old triad of local sensitivity, severe pain, and cold sensitivity. In addition to various clinical trials, imaging studies such
as Radiography, Ultrasonography and Magnetic resonance imaging (MRI) are often helpful in diagnosis. Complete surgery is the treatment of choice to get
complete relief from symptoms and to avoid recurrence. The purpose of this article is to study the Clinical & MRI features of Subungual Glomus tumor in a
41-year-old woman who developed chronic pain in her right ring finger during her daily activities.
Keywords
Hand glomus tumor, Glomangioma, Subungual tumors
Introduction
Glomus tumors are rare malignant lesions arising from a
neuroarterial structure called the glomus body located in the reticular
areas of the hand, accounting for 1% to 4.5% of the tumors in the hand
[1]. The body of Glomus is believed to function in hot regulation. The
general clinical triangle of local soft tissue, severe pain, and sensitivity
to colds significantly favors the glomus tumor.
The average age of presentation ranges from 30 to 50 years,
although it can occur in any age [1].
The glomus body can develop hypertrophy that appears as yellow
or purple under the nail bed. Glomus tumors are usually isolated, but
many lesions have been associated with type 1 neurofibromatosis [3].
The aetiology of glomus tumors is unknown and may be related
to gender, age, trauma, or heredity. Some authors have suggested that
a deficiency in glomus structure can lead to functional hypertrophy
after trauma [3]. The first reported case of glomus tumor was by
Masson in 1924 [4], a few studies have reported glomus tumors, its
pathophysiology and management.
Case Report
A 41-year-old woman has been given a history of severe pain at
the tip of her right ring finger, whenever she applied pressure to the
volar tip during her daily activities for the past three years with a cold
sensitivity. She has visited several different health care providers in the
past, with various diagnoses listed in her medical records including
neuroma, radiculitis, Raynaud’s event, and reversible reactions. There
are no formal systemic complaints.
A physical examination revealed that the digit did not change color
and that the nail appeared normal. There is no apparent difficulty but
of pain relief by applying pressure to the central pulp. Radiographs
and standard laboratory results were within normal limits.
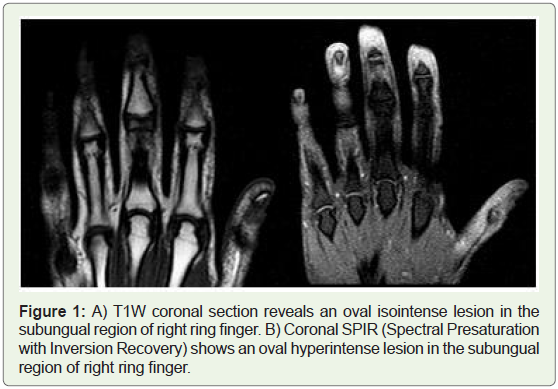
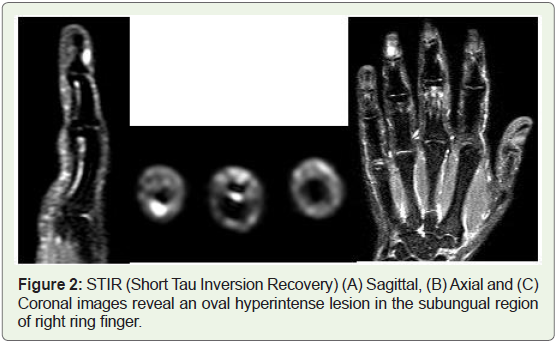
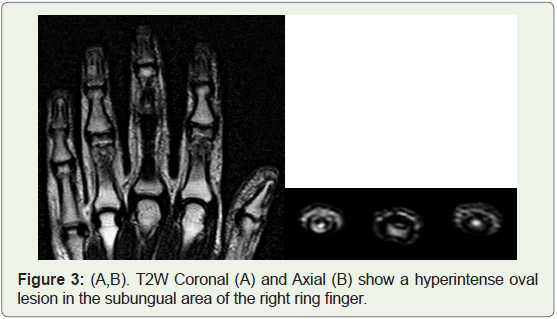
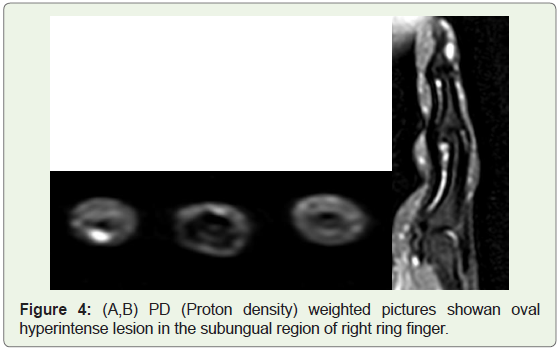
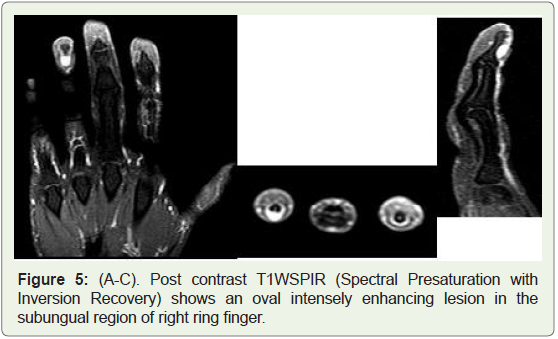
An MRI scan revealed an oval T1W isointense, T2W / STIR
/ PDFS / SPIR hyperintense lesion measuring 6 x 5.3 mm in the
subungual area of right 4th finger. In the T1W fat sat post-contrast
pictures, the tumor showed significant contrast enhancement. In
Computed Tomography imaqes there is no bone erosion in the distal
phalanx. In the USG examination there is an isoechoic wound with
no additional vascularity in color flow studies.
Discussion
Different types of tumors can affect the subungual area,
including solid tissues (glomus tumor, subungual exostosis, softtissue
chondroma, keratoacanthoma, hemangioma, lobular capillary
hemangioma), benign lesions cystic (epidermal and mucoid cysts),
and malignant tumors (cell carcinoma, malignant melanoma [10].
Glomus tumors are rare, benign, and vascular neoplasms arising
from the glomus body which is a contractile neuromyoarterial
structure found in the reticular dermis. The Glomus body contains
the afferent arteriole, anastomotic vessel known as the Sucquet-
Hoyer canal, primary collecting vein, intraglomerular reticulum,
and capsular portion [6]. This structure regulates blood pressure and
temperature by regulating blood flow to the cutaneous vasculature
[7-9]. Although glomus tumors can affect any part of the body, up
to 75% of the hand, and about 65% of these are found on the fingers,
especially in the subungual area. The prevalence of glomus tissue is
approximately equal to that of men and women [11, 12].
Clinical features include excruciating pain, intense tenderness
that may be provoked by mild trauma, and temperature sensitivity.
The nail may be discolored & ridged due to tumour in the subungual
area [6, 11].
Although, the cause of pain in glomus tumor is not well understood,
several hypotheses have been made; the presence of a capsule,
sensitive to stress, the presence of mast cells releasing substances such
as heparin, histamine and 5-hydroxytryptamin that produce pressure
and sensitive heat receptors [13]. In addition, overuse of the nerve
fibers that do not have myelinited nerve fibers that penetrate glomus
tumors has been suggested as a cause of pain [14]. Glomus tumors are
usually found clinically. In addition to the classic presentation, Love’s
pin tests, Hildreth tests, trans-illumination tests and cold-sensitivity
tests are helpful in diagnosing these lesions [3,15].
Radiological Imaging plays an important role in identifying and
classifying subungual tumors because of their small size, indirect
clinical manifestations, and the importance of their function. Recent
research emphasizes the use of studies such as ultrasound & MRI, to
assist in diagnosing and planning surgical management [16, 17].
As the tumor is external to the bone, there may be no radiographic
findings as bone involvement is less common than soft tissue
involvement. Bone changes adjacent to the tumor, caused by pressure
erosion include shallow well corticated osseous defect involving the
distal phalangeal tufts [18].
The MR imaging features considered diagnostic of glomus
tumor include moderate or low signal intensity in T1-weighted
images, high intensity marked in T2-weighted images, and strong
enhancement after gadolinium-based contrast injection (Fig. 5 A-C).
MR angiography is a useful non-invasive supplement to normal MR
imaging to detect glomus tumor. Typical findings of MR angiography
include areas of strong development in the arterial stage and tumor
blush, which increases in size in the delayed stage [6, 12].
In Ultrasound, the glomus tumor usually appears as an hypoechoic
mass under the nail with hypervascularity in the color doppler study
specific for the diagnosis [11, 19,20].
In the analysis of histology, the glomus tumor appears as
endothelium-containing arteries enclosed by a series of circular
epithelioid cells that have a specific tendency to take the form of
spinning [21].
The imaging features of glomus tumors are similar to those of
hemangiomas and are usually not detected before surgery.
Hemangiomas are highly concentrated in the papillary dermis
and epidermis, usually with well-defined margins but may show
invasive margins and usually have a intermediate signal intensity
in T1-weighted images and a high signal intensity in T2-weighted
images. Parts of the blood vessels produce heterogenous signal
intensities with a snake pattern and flow void artifact in T2-weighted
images. Low signal strength in T1- and T2-weighted images can be
caused by phleboliths, calcification, or fibrosis. Contrast enhanced
MR imaging reveals the serpentine or lattice like enhancement of the
lesion [6, 22,23,24].
Subungual Lobular capillary hemangioma is a benign vascular
neoplasm of the skin and a mucous membrane that may occasionally
appear inside the vessels or under the skin [25]. In MR imaging,
the lesion is isointense in T1-weighted images and hyperintense in
T2-weighted images, with marked enhancement after injection of
contrast 25, 26, 27].
Subungual exostosis, also known as Dupuytren exostosis, is a
rare, isolated, malignant lesion from the distal phalanx under the nails
[28]. MR imaging is the best radiologic method to show the effect of
subungual exostosis on surrounding structures and to differentiate
between this lesion and osteochondroma. The fibrocartilaginous cap
in subungual exostosis is hypointense on all MR imaging sequences,
while hyaline cartilage in osteochondroma has high signal intensi (Figure 1-6).
Conclusion
Diagnosis of glomus tumor can be made clinically based on
history taking and clinical examination. Magnetic Resonance Imaging
is required to ensure further diagnosis and management of surgery.
References
8. Kale SS, Rao VK, Bentz ML (2006) Glomus tumour of the index finger. J Craniofac Surg 17: 801-804.
15. Netscher DT, Aburto J, Koepplinger M (2012) Sub ungual glomus tumor. J Hand Surg Am 37: 821-823.
Citation
Kumar MK, Priyadharshini V, Varma RR. Subungual Glomus Tumour of Right Ring Finger; MRI Features. Indian J Appl Radiol. 2021;7(1): 169.