Case Report
Primary Sternal Tuberculosis: A Case Report
Najioullah D*, Laachir G, El Aoud FZ and Chat L
Radiology Department, Cheikh Zaid Universitary Hospital, Rabat Morocco
*Corresponding author: Najioullah D, Department of Radiology, Cheikh Zaid Universitary Hospital, Rabat Morocco,
Email: doubikad@gmail.com
Copyright: © 2021 Najioullah D, et al. This is an open access article distributed under the Creative Commons Attribution
License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is
properly cited.
Article Information: Submission: 04/07/2021; Accepted: 11/08/2021; Published: 14/08/2021
Introduction
Sternum is one of the least common bones of the body to get
infected. Sternal osteomyelitis accounts for less than 2% of cases of
osteomyelitis [1-4]. Sternal involvement is often caused by reactivation
of a latent focus by lymphatic dissemination or hematogenous.
In some cases, it is due to an extension direct from mediastinal
lymphadenopathy [5].
Tuberculous sternal osteitis is usually achronic osteitis with
a long diagnostic delay [1,6]. It manifests as pain and/or swelling
slowly progressing to worsening [6]. Undiagnosed, it is complicated
by abscess of the soft tissues and fistulization, sometimes complicated
by pathological fracture [6,7]. SV is often increased. The tuberculin
skin test is neither sensitive nor specific [1,2]. Standard x-ray may
be normal in the early stages or show uncharacteristic images such
as osteolysis, periosteal reaction, soft tissue opacity or pathological
fracture [2]. Computed tomography is an excellent test for delineating
sternal involvement and extension of the abscess in the soft parts
[4,5]. MRI probably has sensitivity upper to detect early edema of the
marrowbone and soft tissue involvement [5,6]. Diagnosis of sternal
tuberculosis remains difficult in the absence of other pulmonary
or extrapulmonary lesions suggestive of tuberculosis, especially
since other conditions may have the same clinical appearance and
radiological such as a malignant tumor, a localization secondary or
malignant hemopathy [7,8]. Therefore, the ultrasound guided or
surgical biopsy is found indicated in the majority of cases to establish
a histological and/or bacteriological diagnosis [2,3]. However, the
positive microbiological diagnosis is often difficult because of the
alcohol-resistant bacillus from direct examination and after culture
is random [2,3].
Observation
7-year-old child, vaccinated against tuberculosis, who has had
sternal pain for 1 month with small swelling, no other symptoms were
(no fever, no weight loss, no cough ) and no tuberculosis contagion
in the family.
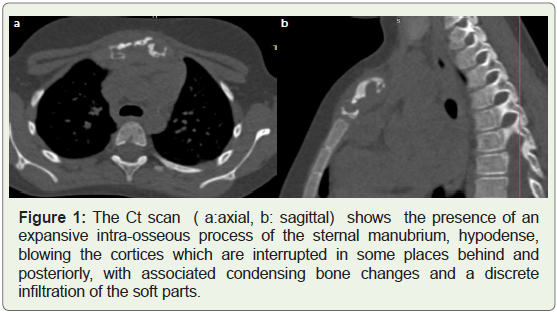
The AP chest x-ray of the sternum revealed sternal lysis. The Ct
show the presence of an expansive intraosseous process of the sternal
manubrium, hypodense, blowing the cortices which are interrupted
in some places behind and posteriorly, with associated condensing
bone changes and a discrete infiltration of the soft parts, extended to
sternoclavicular joint (Figure 1). Fine needle aspiration cytology and
a biopsy of the bone was performed. The anatomopathological study
showed an epithelioid and gigantocellular appearance, with caseous
necrosis, reminiscent of active sternal tuberculosis.
No other tuberculous pulmonary focus or node has been found.
The diagnosis of primary sterna tuberculosis has been retained.
Discussion
Osteoarticular tuberculosis accounts for 1 to 3% of tuberculosis
cases, all locations combined, and involvement of the sternum
represents less than 1% of cases [3,4]. Sternal involvement is
often caused by reactivation of a latent focus by lymphatic or
hematogenous dissemination. In some cases, it is due to direct
extension from mediastinal lymphadenopathy [5]. Tuberculous
sternal osteitis is usually chronic osteitis with a long diagnostic delay
[1,6]. It manifests as pain and/or swelling that slowly progresses to
worsening [6]. Undiagnosed, it is complicated by soft tissue abscess
and fistula, sometimes complicated by pathological fracture [6,7].
The tuberculin skin reaction is neither sensitive nor specific [1,2].
Standard radiography may be normal in the early stages or show
uncharacteristic images such as osteolysis, periosteal reaction, soft
tissue opacity, or pathologic fracture [2].
The computed tomography (CT) scan is an excellent test for
delineating sternal involvementmore sensitive for anatomical
localization and in detecting osseous destruction and soft-tissue
abnormalities [4,5]. MRI is probably more sensitive in detecting early
bone marrow edema and soft tissue involvement [5,6]. The diagnosis
of sternal tuberculosis remains difficult in the absence of other
pulmonary or extra-pulmonary lesions suggestive of tuberculosis,
especially since other conditions can have the same clinical and
radiological appearance such as a malignant tumor, a secondary
localization or a blood disease [7,8]. Therefore, ultrasound-guided
or surgical biopsy is indicated in the majority of cases to establish
a histological and / or bacteriological diagnosis [2,3]. However,
a positive microbiological diagnosis is often difficult because the
isolation of the alcohol-resistant bacillus on direct examination and
after culture is uncertain [2,3].
Treatment of sternal tuberculosis is medico-surgical. Medical
treatment is started as soon as the diagnosis is made [9]. Surgical
treatment may be indicated to drain a cold abscess developed in the
soft tissue [2,4,9]. The prognosis is generally good after treatment.
Sternal TB is predominantly seen in middle-aged adults although no
age is immune and it has also been reported in an infant [6]. It can arise
primarily due to hematogenous route or direct extension from the
hilar lymph nodes and/or could be due to lymphatic dissemination.
Tubercular multiple cutaneous sinuses over the anterior chest wall
may be a manifestation of TB of the internal mammary lymph nodes
spreading along perforators or an extension of tubercular sternal
osteo-myelitis [7,8].
The computed tomography (CT) scan is more sensitive for
anatomical localization and in detecting osseous destruction and
soft-tissue abnormalities. The role of magnetic resonance imaging
(MRI) for detecting early marrow and soft-tissue involvement due
to high contrast resolution [9]. TB osteo-myelitis is characterized
by low signal replacement of the normal marrow fat signal on T1-
weighted images, with high signal intensities on T2-weighted images
and enhancement on T1-weighted images [10].
Possible complications of sternal TB osteomyelitis include
secondary infection, fistula formation, spontaneous fractures of the sternum, compression or erosion of the large blood vessels,
compression of the trachea and migration of TB abscess into the
mediastinum, pleural cavity, or subcutaneous tissues [11-13].
Diagnosis rests largely with the histological and microbiological
examination of sternal tissue. Needle aspiration, as compared to
surgical exploration, is less invasive and may represent the diagnostic
procedure of first choice.
The differential diagnosis of chest wall masses includes pyogenic
infections (Staphylococcus or Streptococcus), malignancy (lymphoma
or metastatic lesions), Brodie’s abscess and granulomatous lesions
or fungal infections (Coccidioides, Histoplasma, Blastomyces or
Cryptococcus).
Conclusion
Tuberculosis of the sternum is a rare form of flat bone tuberculosis.
It is usually a part of disseminated tuberculosis.
The possibility of sternal TB should be kept in mind in the
differential diagnosis of a mass involving the chest wall, particularly
in endemic areas.
References
Citation
Najioullah D, Laachir G, El Aoud FZ, Chat L. Primary Sternal Tuberculosis: A Case Report. Indian J Appl Radiol. 2021;7(1): 166.