Case Report
Left Fourth Branchial Cleft Cyst - A Rare Clinical Entity
Nikam V1* and Kitture B2
1Department of Anatomy, DY Patil Medical College, Kolhapur, India
2I Lab Diagnostic Centre, Ichalkaranji, Kolhapur, india
*Corresponding author:Nikam VR, Department of Anatomy, D.Y. Patil Medical college, Dr. DY Patil Education Society,
Deemed to be University Kasaba Bawada, Kolhapur, India, Tel no: +91-9665730990; E-mail: dr.vasudhanikam@gmail.com
Copyright: © 2021 Nikam V, et al. This is an open access article distributed under the Creative Commons Attribution
License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is
properly cited.
Article Information: Submission: 06/03/2021; Accepted: 23/06/2021; Published: 26/06/2021
Abstract
Fourth branchial arch anomalies are extremely rare and are the result of abnormal development of the branchial apparatus during embryogenesis. They
arise from an incomplete involution of the fourth gill slit during development. Failure to recognize appropriately of these anomalies may result in misdiagnosis.
Here we present a unique presentation of female patient of 21 year old which presented an enlarging painless lateral neck mass. Diagnosis was obtained by
ultrasound imaging.
Keywords
Branchial cleft anomalies; Neck mass; Fourth branchial cleft cyst, Complete surgical excision, Pyriform sinus, Branchial apparatus
Introduction
Branchial cleft anomalies originate from the errors during
embryogenesis, resulting in incomplete involution of branchial clefts.
Fourth branchial cleft cysts are particularly rare accounting for less
than 30% of all branchial arch anomalies [1,2]. The branchial cleft
cyst may originate from the 1st, 2nd and 3rd branchial arch remnants,
however fourth branchial cleft cysts are rare [3,4].
The mean solar time between onset of symptoms and proper
diagnosis seems to be 5 years. Treatment is to excise the cyst and
often combined with partial thyroidectomy that may further decrease
recurrence rates [5].
The incidence rates of types I, II, III and IV are 80%, 95%, 2% and
1-4% respectively with just 100 reported cases. Type IV is reported
very rarely in previous studies. This disease is not linked with gender,
anyhow as claimed by the evidence; it has been reported in females
more than males, at the same time on the reverse some believe that
60% of this disease would happen in males [6].
Of all the fourth branchial cleft anomalies true cysts are particularly difficult to detect as a tract opening is often not identifiable
on endoscopy or contrast enhanced radiography. Moreover while the
number of reported fourth branchial cleft anomaly in the literature
has tripled over the past 20 years [7-11].
Fourth branchial arch anomalies are extremely rare and almost
occur on the left side [12,13]. These anomalies typically present as
recurrent neck infections, abscess, or acute supparative thyroiditis
[14,15]. Imaging is requisite in managing these lesions. For definitive
diagnosis, the relationship of the anomaly to laryngeal nerves must be
confirmed prior to operation [16].
Here we present a rare anomaly of fourth branchial cleft cyst in
a young female.
Case Report
A 21-year-old female was referred to our diagnostic centre for
imaging of swelling on the left side of neck. Patient complained of a
solitary swelling on the left side of neck since one year of duration,
which was incidental on onset and progressively increased since last
four months. She mentioned no change in her voice or suffered from any breathing disorders or dysphasia. In addition, she reported that
there was no history of such similar symptoms for any of her family
members.
On examination patient was a febrile with all parameters within
normal limits. The swelling was visible on the left side of neck
measuring 5 x 3 cm extending about 5-6 cm below mandible. The
mass was anterior and deep to sternocleidomastoid muscle but just
above the clavicle. No abnormalities were noticed in nose, pharynx
and larynx.
On palpation, the mass was soft, mobile and non-tender,
no compressive signs were present. The swelling was anterior to
sternocleidomastoid muscle almost palpable in the midline that
moved with deglutition but was not moving with protrusion of
tongue.
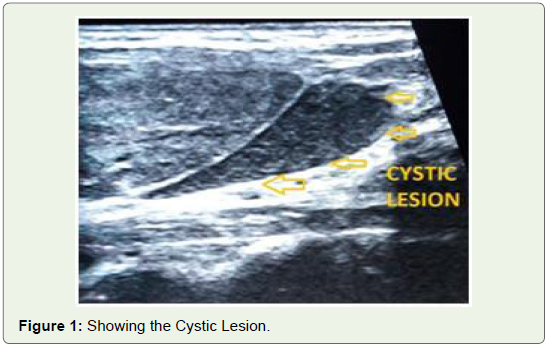
Ultrasound imaging of the neck was done which revealed a cystic
lesion that was measuring 4.2 x 3 x 1.8 cm (Figure 1). It was located
deep to carotid sheath almost in the laryngeal wall (Figure 2).
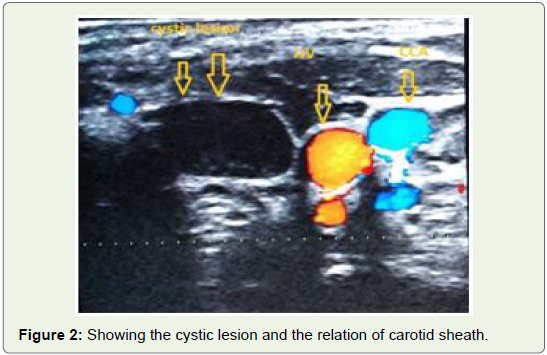
The lesion was well defined anechoic and perilaryngeal in position.
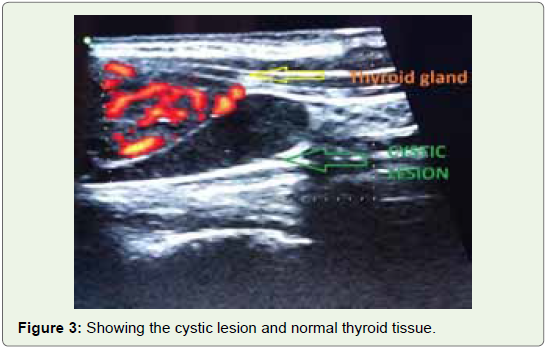
The lesion was located on the left side near midline between thyroid
cartilage and deep to infrahyoid muscle. The thyroid gland appeared
to be normal and thyroid scan showed no functional thyroid tissue in
clinically palpable swelling. The mass was centered in the left carotid
space (Figure 3). The differential diagnosis was confirmed as fourth
branchial cleft cyst.
Discussion
Branchial arch anomalies are the second most common cause
of congenital lesions of the head and neck representing 20% of the
cervical masses [1,3,17,18].
Branchial cleft cyst is a common cause of soft tissue swelling in
the neck of young adult, generally occurs unilaterally and typically
seen in the lateral aspect of the neck. It is clinically apparent in the late
childhood or early adulthood [19,20]. The branchial cleft cyst usually
presents in the second through fourth decades of life [3,15]. However,
in our case the patient was 21 years old.
Fourth branchial cleft anomalies are very rare among branchial
cleft anomalies. Anomalies of the second branchial cleft commonly
called lateral cervical cyst, which are most common and are about
90% [1,9,12,14,16,21]. The remaining 10% are comprised of first,
third and fourth branchial clefts with fourth being the rarest [1,21],
Representing only 1-4% of branchial apparatus anomalies [13,22].
Bilateral cases accounts for 2-3% of the cases [3,23].
The fourth brachial cleft anomaly was described by Sandborn and
Shafer and not until 1981 that Liston theorized the fourth branchial
arch anomaly [7,24]. This anomaly most commonly presents as sinus
tract that course from the apex of pyriform fossa to the upper lobe of
the left side of thyroid gland. This is because fourth branchial arch
anomalies are remnants of the embryological tract, which arises
from pyriform sinus [1,22,24,25]. The tract terminates in the neck
posterior to the internal and common carotid arteries. A fourth
branchial cleft cyst is differentiated from the other types of branchial
cleft cysts through anatomical landmarks; it is bordered laterally
by sternocleidomastoid muscle, medially by trachea, Anteriorly by
common carotid and anteromedial by the strap muscles [24,25].
Four types of branchial cleft cysts are as follows -
♦ Type-I: is often superficial and located on the anterior surface
of sternocleidomastoid muscle deep to platysma. However,
it’s not connected to the carotid sheath. The incidence rate is
8%.
♦ Type II: is most common and the incidence rate is 95% and
located anterior to sternocleidomastoid muscle and posterior
towards submandibular gland and lies lateral to carotid
sheath.
♦ Type III: it is located between the bifurcation of internal and
external carotid arteries lateral to the laryngeal wall. The
incidence rate is 2%.
♦ Type IV: It is located deep to carotid sheath almost in the
laryngeal mucosal space and would open to the larynx.
Such type of cyst emerges as neck mass, abscess and acute
thyroiditis; therefore, some authors suggest that the possible
existence of branchial archanomalies should be considered
in all thyroiditis cyst [3,23]. The patient in this case suffered
from type IV branchial cleft cyst.
Patients with fourth branchial cleft cyst usually presents
with a painless lateral neck mass along the anterior border of the
sternocleidomastoid muscle and most commonly located on the left
side [1,6]. It was positively seen in our case.
A predilection for the left side is likely attributable to an
embryologic tendency for vascular development in left hemi thorax
and diminished growth of right ultimo branchial body [7]. Spread of
infection usually occurs to the left thyroid lobe and causes supparative
thyroiditis that reflects the tracts intimate relationship with the
thyroid gland [7,27].
Third and fourth branchial cleft anomalies are differentiated
anatomically by their relationship to the superior laryngeal nerve,
with third cleft anomaly above and fourth cleft anomaly below [17].
Diagnosis of the fourth branchial cleft cyst anomaly can be made
easily by imaging techniques such as CT, MRI or Ultrasonography
being the modality most commonly used [1,28]. In our case, diagnosis
was dome on ultrasonography imaging.
Although most of the branchial cleft anomalies appear as sinuses
or fistulae, true cyst have been described as well [7,10,1126]. In our
case, it appeared to be true cyst.
The most common treatment for the fourth branchial cleft cyst
is complete surgical excision due to risk of infection or obstruction
[1,28,29].
In our case patient was referred to Department of Surgery where
complete surgical excision of the cyst was done successfully. Post
operatively patient was comfortable.
Conclusion
Although fourth branchial cleft cysts are rare, their existence has
to be kept in mind when dealing with the patients presenting with
neck mass. As it shows fascinating aberrations of foetal development,
a proper preoperative evaluation should be done. Definitive
management is achieved by complete surgical excision.
Acknowledgement
Thanks to Chancellor, Vice Chancellor, Pro-Vice-Chancellor,
Dean of the Medical College, D.Y. Patil Medical College, Kolhapur.
Dr B S Kitture; Director - Eureka Diagnostic Centre, Kolhapur.
References
Citation
Nikam V, Kitture B. Left Fourth Branchial Cleft Cyst - A Rare Clinical Entity. Indian J Appl Radiol. 2021;7(1): 164.