Research Article
Study of Endovenous Laser Ablation of Varicose Veins at a Tertiary Care Hospital
Niyati Sharma* and Manvendra Swarup Sharma
Shri Ram Murti Smarak Institute of medical sciences, Bareilly, Uttar Pradesh, India
*Corresponding author: Niyati Sharma, Shri Ram Murti Smarak Institute of medical sciences, Bareilly, Uttar Pradesh, India E-mail id-niyati.sharma.1990.ns@gmail.com
Copyright: © 2021 Sharma N, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article Information: Submission: 24/11/2020; Accepted: 04/01/2021; Published: 09/01/2021
Abstract
Background: Endovascular Laser Ablation (EVLA) is performed by placing the selected ablation device into the saphenous vein, usually by ultrasound guidance. The ablative device causes endovascular heating, which damages the venous endothelium leading to fibrosis and thrombosis. Benefits of endovascular treatment over surgery include: not needing to make an incision at the thigh and ankle; shorter hospital stays; quicker return to work times;
less post procedure pain; and similar long-term efficacy rates as surgery. Present study was planned to assess endovascular laser ablation of varicose
veins in a tertiary care hospital.
Material and Methods: This prospective study was conducted in patients with varicose veins caused by Saphenofemoral Junction (SFJ)
incompetence with Great Saphenous Vein (GSV) reflux and/or saphenopopliteal junction (SPJ) incompetence or perforator incompetence as demonstrated
by color Doppler.
Results: Present study was conducted in 58 patients diagnosed with varicose veins. Male: female ratio was 2:1. From 58 patients, total 83 limbs were operated. Apart from routine indication other cases were- Venous ulcers (13%), bleeding varicose veins (2%), recurrent varicose veins following surgery (4%) & cosmetic purpose (7%). At 1 month follow-up all patients were examined to rule out any complication. We noted paraesthesia (5.1%),
hyperpigmentation (2%), phlebitis (1%) & haemorrhage (1%) as minor complications. At the end of 6 month, success rate of 93%. Failure was noted in 4 patients; though it was partial they were later treated at same center only.
Conclusion: Patients after treatment with Endovenous Laser Ablation (EVLA) have better recovery with significantly lower post treatment pain, faster return to routine activities.
Keywords
Varicose veins; Endovenous laser ablation; EVLA
Introduction
The World Health Organization defines varicose veins of the
lower limbs, as superficial dilated veins that present as enlargements
that are baggy or cylindrical due to a damaged vein valves. In 70%
of cases, saphenous veins are affected. It is reported in 40%-60% of
men and 25%-30% of women [1]. Patients present with a spectrum
of symptoms, including prominent leg veins (telangiectasias,
varicosities), heaviness, pain, itching, swelling, muscle cramps,
discoloration, and ulceration [2].
Various risk factors associated with the condition include
female sex, prolonged standing/sitting, pregnancy, occupation (e.g.,
policemen, farmers, teachers), hormonal influence, obesity, family
history, and advanced age. Different treatment options include
traditional surgical management and newer endovascular treatments.
Endovascular options include thermal ablation, Mechanic-Chemical
Ablation (MOCA), and foam sclerotherapy.
Endovascular Laser Ablation (EVLA) is performed by placing the
selected ablation device into the saphenous vein, usually by ultrasound
guidance. The ablative device causes endovascular heating, which
damages the venous endothelium leading to fibrosis and thrombosis.
Benefits of endovascular treatment over surgery include: not needing
to make an incision at the thigh and ankle; shorter hospital stays; quicker return to work times; less postprocedure pain; and similar
long-term efficacy rates as surgery [3].
A meta-analysis by Mundy et al demonstrated occlusion rates of
the great saphenous vein in the 88 to 100% range after EVLA [4].
Present study was planned to assess endovascular laser ablation of
varicose veins in a tertiary care hospital.
Material and Methods
This prospective study was conducted in the Department of
Radiodiagnosis, Shri Ram Murti Smarak Institute of Medical Sciences,
Bareilly. Study duration was 1 year. Permission was obtained from
institutional ethics committee.
Inclusion criteria:
1. Varicose veins caused by Sapheno-Femoral Junction (SFJ)
incompetence with Great Saphenous Vein (GSV) reflux and/
or Sapheno-Popliteal Junction (SPJ) incompetence or perforator
incompetence as demonstrated by color doppler.2. Symptomatic varicose veins (symptoms-pain, swelling, itching,
skin discolouration, bleeding, etc.) and the ones with asymptomatic
varicose veins (cosmetic purpose).
3. Recurrence of varicose veins following surgery and ones with
non healing venous ulcers.
4. Patients willing to participate in study & follow up.
Exclusion criteria:
1. Patients with Deep vein thrombosis,2. Pregnant females,
3. Patients with intrinsic reflux in deep veins were excluded from
the study.
A written informed consent was taken from patients for
participation in present study. A general examination was performed
which included history, physical examination and color Doppler of
lower limb veins. All the patients were examined on Acuson Juniper
SS0627 ultrasound system, the length and diameters of the veins were
recorded.
The following points were included in color Doppler examination
of the lower limb venous system
The following points were included in color Doppler examination
of the lower limb venous systema.
a. Deep vein status
b. Sapheno-femoral junction reflux (Grade 1-4)
c. Superficial veins-Great Saphenous Vein (dilated/not dilated)
d. Sapheno-popliteal Junction reflux
e. Short Saphenous Vein (dilated/not dilated)
f. Perforators (competent/incompetent)
g. Deep venous system patency.
Necessary laboratory workup was done. Patients & relatives
counseled & procedure was explained in detail. After clinical and
imaging studies patients were taken for the procedure. Color Doppler examination was performed on table to confirm all findings. EVLA
was done by using Biolitec laser machine (1470 nm wavelength).
The lasers themselves come in two varieties, continuous wave and
pulsed, with the latter generally being more powerful. Various laser
wavelengths have been used for ablation including the 1470 nm, 810
nm, 940 nm, 980 nm, 1064 nm and 1320 nm. The primary target
chromophore of the 810 nm and 940 nm lasers is haemoglobin,
while the higher wavelength lasers primarily target water. During
the procedure, the laser fiber is drawn down the vein in a stepped
or continuous fashion with the laser firing continuously or in onesecond
pulses. The dose of energy delivered is reported as the Linear
Endovenous Energy Density (LEED), in joules per cm of vein (J/
cm), or as fluence, which is the energy delivered per surface area (J/
cm2). Controversy exists over the minimum energy needed to achieve
optimal occlusion rates, but levels of 60 J/cm or higher are considered
adequate. The occurrence of treatment failures above these doses,
however, suggests that other factors influence treatment success
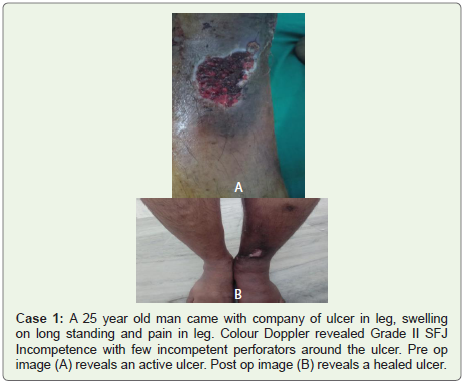
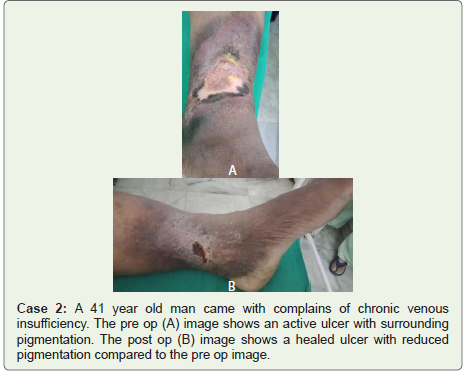
(cases 1-3).

All aseptic precautions were taken. Local anesthesia in the form of 2% Lignocaine was given and Ultrasonogragphy (USG) guided puncture of the dilated superficial vein was done. After free backflow
of blood into the needle, a guidewire was passed into the vein and pushed upto the SFJ. Then a long sheath (6 Fr) was pushed over the guide wire and the guide wire was then removed. Correct positioning
of the sheath and the inserted laser fiber within was done under USG guidance i.e. 2 cm away from SFJ to avoid deep vein ablation. Tumescent anesthesia i.e. 15 cc of 2% Xylocaine + 10 cc of sodium bicarbonate + 5 cc sensorcaine in 300 ml normal saline was given around the vein under USG guidance. Using appropriate energy and power, ablation of the veins was done. Post ablation USG was done to confirm complete occlusion of dilated veins, incompetent perforators and to check patency of deep veins. Class II compression stockings
(i.e. one with a gradient of 30-40 mm Hg) were applied to the limb upto the groin.
After observation for 30 minutes patients were shifted to ward, routinely patients were re-examined & discharged after 2 days Patients were asked to follow up at 1 week, 1 month, 6 months, 1 year
and then yearly. Patients were instructed to wear the stockings for 48
hours continuously and thereafter in day time and during physical
activity for a period of 6 months. All data collected in a proforma,
analyzed in Microsoft excel.
Results
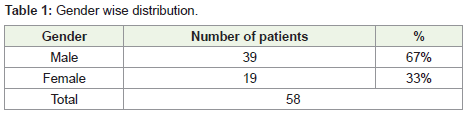
Present study was conducted in 58 patients diagnosed with varicose veins. Male (67 %) patients were more than female (33 %). Male: female ratio was 2:1 (Table 1).
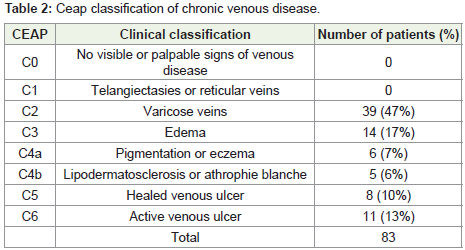
From 58 patients, total 83 limbs were subjected to Endovenous Laser Ablation. We classified chronic venous disease by CEAP (Clinical-Etiology-Anatomy-Pathophysiology) classification. Most common type was C2-Varicose veins (47%), others were C3-Edema (17%), C6-Active venous ulcer (13%), C4a-Pigmentation or eczema
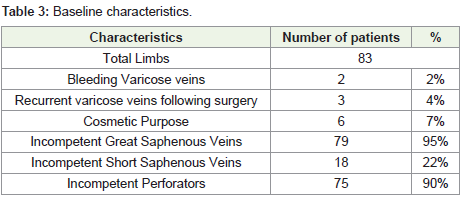
(7%), C4b- Lipodermatosclerosis or athrophie blanche (6%) & C5- Healed venous ulcer (10%) (Table 2).
bleeding varicose veins (2%), recurrent varicose veins following surgery (4%) & cosmetic purpose (7%). On colour doppler assessment we noted incompetent great saphenous veins (95%), incompetent perforators (90%) & incompetent short saphenous veins (22%) as prominent findings. Incompetent perforators generally have >3
mm size and they shows reflux on ultrasound. These are assessed in standing position. EVLT of perforators is done using the baretip fiber of laser machine (Table 3).
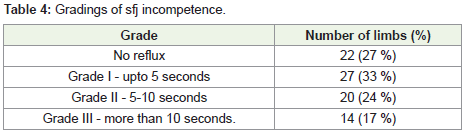
We also assessed incompetence at sapheno-femoral junction.
Normally there should be no reflux or <0.5sec if seen. The longer the
duration of reflux or the greater the reflux time implies more severe
disease. We noted no reflux in 27 % limbs. 33 %, 24 % & 17 % limbs
had SFJ incompetence of grade I,II & III respectively (Table 4).
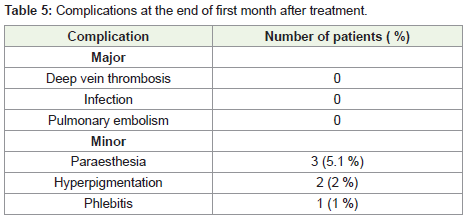
At 1 month follow-up all patients were examined to rule out
any complication. Out of 11 ulcer patients healing was noted in
10 patients (91 %). We did not noted any major complication like
infection, deep vein thrombosis & pulmonary embolism. We noted
paraesthesia (5.1 %), hyperpigmentation (2 %) & phlebitis (1 %) as
minor complications. At the end of 6 month, success rate of 93 %.
Failure was noted in 4 patients; though it was partial they were later
treated at same center only (Table 5).
Discussion
Currently there are two ways for varicose vein management:
lifestyle modifications and medical procedures. Lifestyle-related
recommendations include the avoidance of a prolonged standing and
sitting, an intensification of physical exercise, a loosening of restrictive
clothes, and losing weight by obese people5.Medical methods include
the use of venoactive drugs, compression treatment, sclerotherapy,
phlebectomy, open venous surgery with ligation and stripping, and
endovenous ablation techniques [6,7].
Regarding prophylactic issues, Robertson et al. did not find
any good-quality studies that would enable assessment of whether
lifestyle modifications might be useful as prophylaxis and for avoiding
complications of varicose veins [8]. Chronic venous disease is
associated with depression in up to 30% of patients [9]. Assessment of
the Quality-of-Life is essential and integral allowing a thorough and a
complete evaluation of the condition. Improvement or deterioration
in the disease is associated with a change in the patient’s QoL score.
Several tools are available to assess Quality-of-Life [10].
Experiments showed that EVLA is less stressful for endothelial
cells than CVS, as the serum obtained from patients undergoing this
procedure fueled their proliferation and reduced senescence and
oxidative stress. This improved functionality of endothelial cells upon
EVLA, in particular decreased senescence, is of special importance
with respect to the spreading of the pathology within normal vessels,
of which conclusion stems from the histopathological analysis by
Aunapuu and Arend showing that endothelial cells from varicose
patients display specific discontinuity and denudation that may be a
manifestation of cellular senescence [11].
Kheirelseid et al. in their meta-analysis noted that 36.6% patients
who underwent EVLA presented with recurrence in comparison with
33.3% patients who underwent conventional surgery at the end of
5 years [12]. Xiao et al. found no difference in the results of EVLT
versus surgery.49 one study showed that 50% of recurrences occurred
after 2 years of surgery whereas recurrence was seen in 12% of patient
within 6 months of laser ablation [13,14]. We noted recurrence in 7%
patients at the end of 6 months.
Studies comparing surgery and endothermal procedure found
both to have the same results over the long term; however, the
endothermal procedure had several advantages, including it being
a safe and effective procedure with faster recovery [15]. RFA and
laser ablation had similar outcomes on both short-and long-term
follow-up. Several studies have found minimally invasive procedures as effective and safe with one study reporting endothermal ablation
being superior to surgery [16-18].
A meta-analysis reported that the outcome and recurrence
rate after EVLA was equivalent to those of conventional surgery
or sclerotherapy. EVLA and RF are very useful as they have fewer
complications, less pain and allow quicker return to normal activities.
Therefore, EVLA of the GSV is recommended as safe and effective
treatment of saphenous incompetence [19]. Comparative studies in
which the outcomes of patients undergoing Classic Vein Stripping
(CVS) and EVLA were analyzed revealed that the latter experienced
lower postoperative pain and bleeding, decreased frequency of wound
infections and hematoma, and shorter time of convalescence [20].
Endovenous Laser Ablation (EVLA) has the advantage of nil or
minimum hospital stay, less pain and discomfort, early return to
work, minimum surgical hazards thus lesser chance of adverse effects
like bleeding or abrasion [21].
Conclusion
Patients after treatment with Endovenous Laser Ablation
(EVLA) have better recovery with significantly lower post treatment
pain, faster return to routine activities. EVLA has better treatment
success rate & significantly less incidence of post-operative infection,
paresthesis, hematoma and pain.
References
Citation
Sharma N, Sharma MS. Study of Endovenous Laser Ablation of Varicose Veins at a Tertiary Care Hospital. Indian J Appl Radiol. 2021;7(1): 156.