Research Article
Role of Chest Radiography for evaluation and Severity Scoring in COVID-19 Pneumonia
Parate R1, Tiwari S1*, Parate T2 and Anand A1
1Government Medical College and Hospital, Medical Square, India
2Indira Gandhi Government Medical College and Hospital, India
*Corresponding author: Tiwari S, MBBS, MD Radiodiagnosis(ongoing), Government Medical College and Hospital, Medical Square, Nagpur, Maharashtra, India- 440003, Mailing address- 2, Shastri Layout, Subhash Nagar, Jaitala Road, Nagpur-440022, India, Ph. No. 9096710110; E-mail- shreeya.13.tiwari@gmail.com
Copyright: © 2020 Parate R, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article Information: Submission: 22/10/2020; Accepted: 04/12/2020; Published: 07/12/2020
Abstract
Objective: 1. Analysis of radiographic features of Covid-19 pneumonia upon initial presentation to the Emergency Department (ED).
2. Exploring the prognostic utility of chest radiograph by means of a semi-quantitative severity scoring system (modified RALE scoring) for patients with
COVID-19 pneumonia.
Materials and methods: In this retrospective study, patients presenting to two tertiary care center EDs with COVID-19 confirmation on real-time Reverse Transcriptase Polymerase Chain Reaction (RT-PCR) were identified. For these patients, the clinico-epidemiological data was recorded and chest radiograph was performed. Each patient’s radiograph was divided into 6 zones and examined for opacities. Both lung scores were collated into a total concordant severity score (0 to 8). Correlation between clinical status and radiological severity was looked for.
Results: Of the 1000 patients who had a positive RT-PCR for COVID-19, 611were males (61.1%) and 389 females (38.9%), with a mean age of 45.54 years (range 8-96 years). 423 (42.3%) patients were asymptomatic and 433(43.3%) chest radiographs had no radiological thoracic involvement. In the radiologically positive group, commonly observed alterations included: 397 patients (69.7%) with alveolar opacities, 191(33.5%) with consolidation,
62(10.8%) with diffuse radio-opacities and 100(17.5%) with coexistent alveolar opacities and consolidations. Peripheral (41.1%) and bilateral (76.08%) distribution of opacities was most striking. Chi 2 test showed a significant correlation between modified RALE scores and patient’s symptoms. Higher modified RALE score strongly correlated with symptomatic disease (Chi= 133.93, p<0.001).
Conclusion: Chest radiograph in COVID 19 pneumonia shows alveolar opacities or consolidation with peripheral and bilateral predominance. Modified RALE score can be used in the emergency setting as a semi-quantitative tool for prediction of clinical severity which is a direct indicator of disease outcome.
Keywords
COVID-19; Clinical features; Chest radiograph pattern; Modified RALE scoring
Abbreviations
COVID-19: Coronavirus Disease-19; SARS-CoV-2: Severe
Acute Respiratory Syndrome Coronavirus 2; RT-PCR: Reverse
Transcriptase Polymerase Chain Reaction; RALE: Radiographic
Assessment of Lung Edema; ED: Emergency Department; CT:
Computed Tomography; COPD: Chronic Obstructive Pulmonary
Disease; HMIS: Health Management Information System
Introduction
At the end of 2019, a novel virus SARS-CoV-2 (Severe Acute Respiratory Syndrome Coronavirus 2) expanded globally from China with the first Indian cases dating back to January 2020 [1]. The disease
outbreak in India paced up by the end of May 2020 with the total confirmed cases being 5,562,663 as on September 22, 2020 [2]. This new coronavirus causes a highly infectious disease, commonly called Coronavirus Disease 19 (COVID-19): Lung infection presents with severe pneumonia to more Aggressive acute Respiratory Distress Syndrome (ARDS) [3,4]. Genetic sequencing of SARS-CoV-2 has enabled the use of Real-Time Reverse Transcription Polymerase Chain Reaction (RT-PCR) for detection of viral nucleic acid, and nowadays this is the diagnostic gold standard [3]. However, this
serologic test has several limitations due to the high number of falsenegatives and delayed results. Radiological evaluation of patients with clinical-epidemiological suspicion of COVID-19 is indispensable, especially in the Emergency Department (ED) while waiting for RT-PCR results, to have a rapid evaluation of thoracic involvement.
The recent COVID-19 radiological literature focuses primarily on Computed Tomography (CT) which is more sensitive and specific than chest radiograph. In particular, in China, CT was used as a first-line diagnostic method for COVID-19 [5]. However, it must be remembered that performing CT scan has its setbacks during this pandemic, ranging from excessive radiation exposure especially to younger patients to the mandatory scanner disinfection procedures. Thus most Indian centers are employing chest radiograph as the firstline method producing faster results compared to those of RT-PCR, especially by using portable X-ray units which reduce the movement of patients and minimize the risk of cross-infection [6-8]. Thus, the purpose of our study is to describe the main radiographic findings in a selected cohort of patients and to correlate the radiological severity with patient’s clinical state which is directly related to patient hospitalization or discharge.
Materials and Methods
Ethics:
The study was approved by the review board of the institutions
and requirement for informed consent was waived since the study
had no risk and would not adversely affect the subjects’ rights or
welfare. Patient selection for this study was consecutive, and no
exclusion criteria were applied.Selection and description of participants:
Chest radiographs of patients with clinico-epidemiological
suspect of COVID-19 infection performed at the ED of two tertiary
care centers in central India from May 30 to August 30, 2020, were
retrospectively reviewed. RT-PCR nasopharyngeal-throat swab and
chest radiographs were performed immediately at the ED access and
clinical-epidemiological data was recorded for COVID-19 infection
(fever, cough, dyspnea, respiratory impairment, diarrhea, myalgia and
dysgeusia). RT-PCR results were considered the reference standard.
For radiological assessment, we selected only patients with RT-PCRpositive
results. The outcome was expressed in terms of the correlation
between radiological severity and disease symptomatology.Technical information:
All chest radiographs were acquired as digital radiographs
with the portable X-ray unit (Allengers and Samsung, Korea) in
the isolation wards in the postero-anterior or antero-posterior
projection. All images were stored in a data portal, HMIS (Health
Management Information System) [9]. A retrospective review of
each radiograph was performed to define the predominant pattern of COVID-19 pneumonia presentation in patients with a positive
RT-PCR. Radiographic features including consolidation, alveolar
opacities, pulmonary nodules and diffuse radio-opacities were
diagnosed according to the Fleischer Society glossary of terms [10].
Moreover, chest radiographs were assessed for the presence of a
specific distribution of the disease (mostly peripheral or perihilar
predominance), monolateral (right or left lung) or bilateral disease
or diffuse predominance. All thoracic images were also assessed for
evidence of other associated pulmonary pathology (pleural effusion,
pneumothorax).Radiograph scoring:
Radiographic Assessment of Lung Edema score (RALE score)
was initially proposed by Warren et al. The radiograph was divided
into four quadrants. Each quadrant was assigned a consolidation
score (0 to 4) to quantify the extent of alveolar opacities and a density
score (1 to 3) for more quantitative assessment of the density of
opacification by quadrant. The final RALE score was the product of
the consolidation and density score for each quadrant ranging from 0
(no infiltrates) to 48 (dense consolidation in >75% of each quadrant)
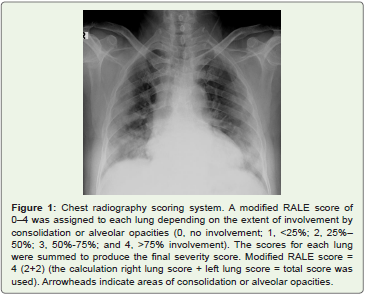
[11].In our study, a simplified and modified RALE score of 0-4 was
assigned to each lung depending on the extent of involvement by
consolidation or alveolar opacities (0, no involvement; 1, <25%
involvement; 2, 25%-50% involvement; 3, 50%-75% involvement; 4,
>75% involvement; Figure 1).The scores for each lung were summed
to produce the final severity score from 0 to 8 [12].
Statistics:
Collected data was entered into Microsoft excel software and
coded. Charts and tables were prepared using Microsoft word and
excel software. Descriptive data was presented in frequency and
percentage.The correlation between modified RALE score and presence of
symptomatic disease was performed by Chi2 test. P value < 0.05 was
considered as statistically significant and statistical software STATA
version 14.2 was used for data analysis.
Results
Demographic and clinical data of entire cohort:
1000 patients admitted to Central India’s two tertiary care centers
having confirmed COVID-19 pneumonia were retrospectively
enrolled in our study from 30 May to 30 August 2020. The
demographic and clinical characteristics of patients are summarized
in Table 1. In our cohort, the mean age was 45.54 years (range 8 to
96). There was male predominance (61.10% men and 38.9 % women).
History of contact with positive patient could be traced in 50%
patients. 42.3% patients in our cohort were clinically asymptomatic.
Amongst the symptomatic group, the most common symptoms
at onset were fever, cough and dyspnoea seen in 370, 308 and 283
patients respectively. Other less common symptoms included sore
throat (3.3%), chest discomfort (1.5%), diarrhea (1.2%), haemoptysis
(1%) and miscellaneous manifestations (10.9%). The most common
comorbidity seen amongst patients was hypertension (23.2%)
followed by diabetes mellitus (16.2%), chronic renal disease (2.3%),
COPD (1.4%) and chronic liver disease (0.9%).Radiographic features:
433 patients (43.3%) had no demonstrable radiographic
thoracic abnormality. Figure 2 depicts the distribution of chest
x-ray abnormality in symptomatic and asymptomatic patients. Of
the total asymptomatic patients, 289 (68.32%) showed radiographic
abnormality. This stratum of patients, which otherwise would have been sent home, could be directed for hospitalization due to the
information extracted by a radiograph. In remaining 134 (31.67%)
asymptomatic patients the chest radiograph was normal. 142 (24.8%)
symptomatic patients had no overt radiographic findings and so CT
examination was suggested to uncover the parenchymal changes, if
any.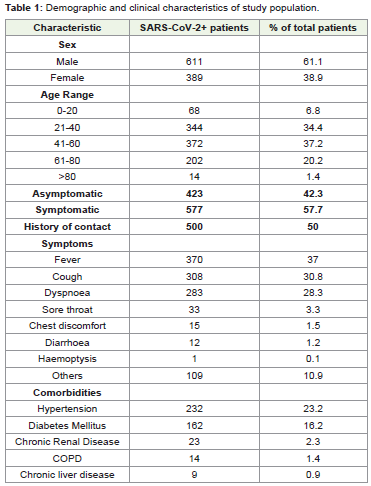

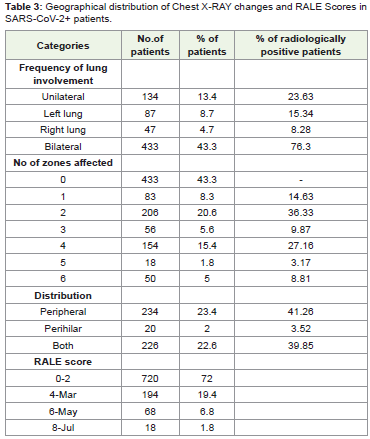
Amongst the radiologically positive group, the typical pattern of radiographic imaging features from our cohort comprised bilateral (76.08%) and peripheral (41.12%) alveolar opacities (69.77%). The following alterations were more commonly observed (Figure 3): 397 patients with alveolar opacities (69.77%), 191 (33.57%) with
consolidation and 100(17.57%) patients with consolidations and alveolar opacities coexistent in the same radiograph. We also found nonspecific signs for COVID-19 pneumonia as pleural effusion (4.74%), nodules (3.16%) and pneumothorax (0.17%). Unilateral disease showed left lung involvement (87 patients, 8.7%) more frequently in our study as compared to the right lung (47 patients; 4.7%). 2 zone involvement (206 patients, 20.6%) was most commonly observed followed by four zone involvement(154 patients, 15.4%). Other radiographic features are described in (Table 2 and 3).

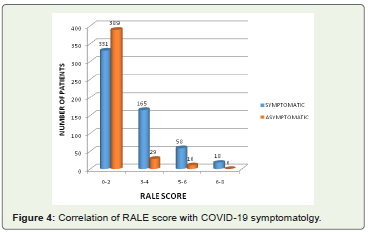
Modified RALE scoring:
Inferences from modified RALE scoring using Chi 2 test
revealed a score of 0-2 in majority of patients (720, 72.0%). Of
these, 389(54.03%) were asymptomatic and 331(45.97%) were
symptomatic. 223 of 262(85.11%) patients with a modified RALE
score of 3-6 had clinical manifestations of disease. As the RALE score increases, there occurs more evident discrimination between symptomatic and asymptomatic groups. Higher modified RALE
score of 6-8 was observed in 18 patients all of whom had symptomatic
disease at presentation and required hospital admission for further
management (Figure 4).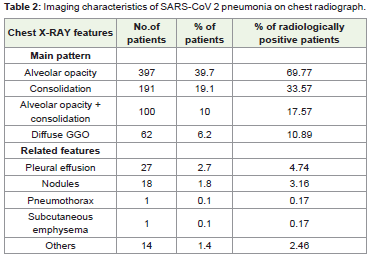
Discussion
The worth of imaging tests relates to the generation of results
that are clinically workable either for establishing a diagnosis or for
guiding management, triage, or therapy. That value is diminished by
costs that include the risk of radiation exposure to the patient, risk
of COVID-19 transmission to uninfected health care workers and
other patients, consumption of PPEs, and need for cleaning and
downtime of radiology rooms in resource-constrained environments
[13]. Chest radiography is widely utilized as a screening tool for
detecting COVID 19 infection. However its prognostic utility has
not been validated in patients with COVID-19. The profitability of
RALE scoring to aid in clinical management has been demonstrated
by other several studies conducted by Cozzi D et al. Fabio Ciceri et
al. Terrance C. et al etc. [14-16]. It is thus recommended to expand
the use of radiographs beyond its present applications, especially in
resource-limited regions.
It is operationally more complex to perform CT scans, especially
considering the disinfection procedures that come into play after each
examination. For this reason, portable X-ray machine is very useful
and inexpensive. Radiographs can be taken at the patient’s bedside
minimizing the risk of cross-infection.
CT must be reserved for additional specific situations: in case
of clinical-radiological discordance, in case of clinical deterioration
and cases of acute complications (i.e. severe respiratory failure or
pulmonary embolism). CT has a high sensitivity (around 97-98%)
but it has a very low specificity in detecting typical features of SARSCoV-
2 pneumonia [13,17,18].
The study has several limitations: The study is retrospective
with lack of a non-COVID-19 control group limiting evaluation of
sensitivity and specificity of chest radiography. The intervals between
serial chest radiographs and RT-PCR testing were dictated by
clinical need and hence were not uniform. Radiologist’s experience
in evaluation of radiographs over HRCT holds an important count
and could be a subject to bias. Follow up evaluation was not done
truncating the correlation with the disease course.
Further research can be directed in this field to effectively
overcome the above drawbacks and more robust guidelines can be
formulated for radiograph based scoring.
Conclusion
In summary, we have described the features of coronavirus
disease 2019 (COVID-19) on chest radiographs and proposed
a severity scoring for rapid triage of patients to aid in appropriate
management. As the COVID-19 pandemic threatens to overwhelm
health care systems worldwide, highlighting the usefulness of a
simple radiograph as a tool for identifying and stratifying cases
ofCOVID-19 is justified. Determination of radiological severity can
aid in effective patient categorization and enforcement of appropriate
clinical management.
References
Citation
Parate R, Tiwari S, Parate T, Anand A. Role of Chest Radiography for evaluation and Severity Scoring in COVID-19 Pneumonia. Indian J Appl Radiol. 2020;6(1): 155.