Case Report
A Rare Case of Late Presentation of Superior Mesenteric Artery Syndrome Following Kyphoscoliosis Surgery
Srijit Saha* and Aarti Anand
Department of Radiodiagnosis, Government Medical College, Nagpur, India
*Corresponding author: Saha S, Department of Radiodiagnosis, Government Medical College, Boys’ Hostel 7, Room 10, Hanuman Nagar, Medical Chowk, Nagpur-440003, India, Phone num: +91 9836018823; E-mail: srijit333@gmail.com
Copyright: © 2020 Saha S, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article Information: Submission: 06/10/2020; Accepted: 03/12/2020; Published: 07/12/2020
Abstract
Introduction: Obstruction of the third part of the duodenum by the Superior Mesenteric Artery (SMA) can occur following surgical correction of scoliosis. The condition most commonly occurs in significantly underweight patients with severe deformities during the first few days to a week following spinal surgery.
Case presentation: We present the atypical case of an adolescent idiopathic thoracolumbar scoliosis that underwent corrective surgery with instrumentation 3 months back. And developed SMA syndrome several months postoperatively. The condition manifested with recurrent vomiting, abdominal distension, marked dehydration, and severe electrolyte disorder. Prolonged nasogastric decompression, nasojejunal feeding, IV fluids and antibiotics with
proper positioning resulted in resolution of the symptoms with no recurrence at follow-up.
Conclusion: SMA syndrome can occur much later than previously reported and with potentially life-threatening symptoms following scoliosis correction. Early recognition of the condition and institution of appropriate conservative measures is critical to prevent the development of severe complications including the risk of death
Keywords
SMA syndrome; Kyphoscoliosis; CT angiography
Introduction
Vascular compression of the third part of the duodenum by the Superior Mesenteric Artery (SMA) results in the development of a rare condition of gastric outlet occlusion known as SMA syndrome [1]. The etiology of the syndrome is connected to the anatomy of the third part of the duodenum in relation to the aortomesenteric angle.
Obstruction of the small bowel by the SMA has been previously
associated with spinal manipulation in the surgical or conservative
management of scoliosis.
In scoliosis, the syndrome occurs most commonly in thin
and asthenic patients with a low Body Mass Index (BMI) who
undergo spinal manipulation and correction of the curvature by
instrumentation, skeletal traction, casting or bracing; these corrective
techniques all result in significant lengthening of the vertebral column
and an extrinsic compression of the distal duodenum as it passes
through the sharp angle formed by the aorta and the spine posteriorly
and the SMA anteriorly. Following scoliosis surgery, the condition
usually develops during the first postoperative week [2].
We present a patient with an adolescent idiopathic kyphoscoliosis
who underwent spinal correction surgery and developed severe SMA
syndrome 3 months following surgery. Such late presentation has not
been reported in literature till date as per our knowledge.
Case Report
A 15 years old female patient came to the Emergency with complain of pain, vomiting and abdominal distension for 15 days and
constipation for 2 days. She is a known case of idiopathic thoracolumbar
kyphoscoliosis. She underwent corrective surgery 3 months
back.
X-ray abdomen AP view showed 1-2 air-fluid levels. There is a
large air-fluid level in the fundic area. Central abdomen was gas less,
however peripheral abdomen showed some gas (Figure 1).
No specific diagnosis could be reached via ultrasonography, as
most of the abdomen was obscured by the fluid and solid mixed
content within the bowel.
The patient was taken for emergency contrast enhanced CT
abdomen & pelvis
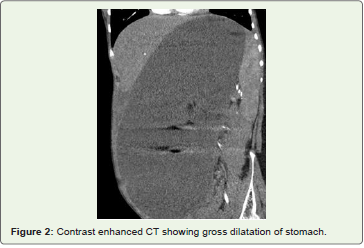
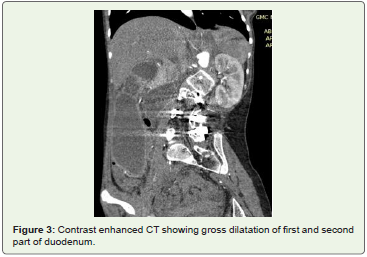
There was gross dilatation of first and second part of duodenum
and gross dilatation of stomach with air-fluid level within the stomach
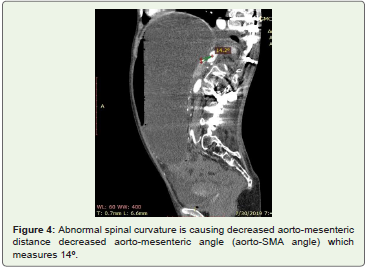
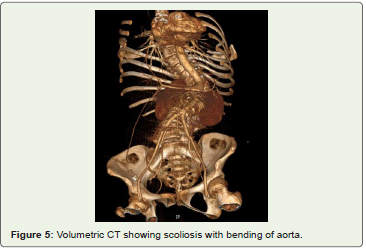
(Figure 2 and 3). Abnormal spinal curvature caused decreased aortomesenteric
distance, measuring 2.5 mm & decreased aorto-mesenteric
angle (aorto-SMA angle) which measured 14º (Figure 4 and 5).
It was diagnosed as a case of duodenal obstruction at D3 segment
due to decreased aorto-mesenteric distance secondary to abnormal
spinal curvature- Secondary Superior Mesenteric Artery (SMA).

Syndrome
Management & followup:
The patient was managed conservatively with nasogastric decompression, nasojejunal feeding, IV fluids and antibiotics; and proper positioning was given. She was discharged when the symptoms subsided, was advised for a balanced diet. She is now well with no such complaints at present.Discussion
So, here we presented an atypical case of a patient with adolescent idiopathic thoracolumbar scoliosis who underwent corrective surgery with instrumentation 3 months back. She developed SMA syndrome due to progressive weight loss several weeks postoperatively. The condition manifested with recurrent vomiting, abdominal distension, marked dehydration, and severe electrolyte disorder. Prolonged nasogastric decompression, nasojejunal feeding, IV fluids and antibiotics with proper positioning resulted in resolution of the symptoms with no recurrence at follow-up.
Superior Mesenteric Artery (SMA) syndrome [1,2], also known
as Wilkie syndrome, is a rare acquired vascular compression
disorder in which acute angulation of the Superior Mesenteric Artery
(SMA) results in compression of the third part of the duodenum,
leading to obstruction. Fat and lymphatic tissues around the SMA
provide protection to the duodenum against compression. Under
conditions of severe weight loss like anorexia nervosa, malabsorption,
hypercatabolic states (burns, major surgery, malignancy), this cushion
around the SMA is diminished, causing angulation and reduction in
the distance between the aorta and the superior mesenteric artery.
Other conditions may also precipitate this syndrome: increased
spinal lordosis, application of a body cast, short ligament of Treitz,
multiple attachments of the ligament of Treitz to the duodenum, high
fixation of the duodenum by the ligament of Treitz, associated with
diabetes mellitus and blunt abdominal trauma, as a Complication of
spinal Surgery, etc.
CT and Magnetic Resonance Angiography (CTA/MRA)
enable visualization of vascular compression of the duodenum and
measurement of aortomesenteric distance [3-6]. Normally, the
aortomesenteric angle and aortomesenteric distance are 18-70° and
10-28 mm, respectively. In SMA syndrome, both parameters are
reduced, with values of 6° to 15° and 2 to 8 mm respectively.
The incidence of SMA syndrome after surgical procedures to
correct spinal deformities has been reported to vary between 0.5 and
4.7% [2,7-11]. This occurs in early post-operative period, within a
week or two. Children usually present for surgical correction of an
adolescent idiopathic scoliosis during the phase of their most rapid
longitudinal growth. The mechanism is that of an acute lengthening
of the spinal column, which results in a cephalad displacement of
the aorto-SMA junction at the expense of lateral mobility, due to
either rapid height gain occurring during adolescence, or following
correction of spinal deformities using either conservative (body casts
and braces) or surgical methods. This accelerated skeletal growth may
alter the relation between the SMA and the spine by decreasing the
aortomesenteric angle and, therefore, increase the risk for duodenal
compression.
Certain factors has been attributed to delayed onset SMA
syndrome in postoperative patients like that mentioned in this case
report [ 2,10,11].
1. Progressive postoperative weight loss
2. The application of the spinal jacket could have caused extrinsic pressure to the abdomen, resulting in further decrease in the aortomesenteric angle and contributing to the onset of the symptoms.
3. In addition, disruption of the autonomic nerve supply to the small intestine, which commonly occurs during the retroperitoneal dissection to approach anteriorly the thoracolumbar spine, can precipitate the development of the condition [7].
Conclusion
We believe that it is essential to identify those patients who are
at greater risk of developing duodenal obstruction. Initiate intensive
preoperative dietary supplementation in undernourished patients
scheduled to undergo spine deformity surgery as a preventative
measure. We have described a patient who demonstrates that SMA
syndrome can develop late following scoliosis surgery. A high
index of suspicion will lead to an early diagnosis of the condition
at a stage when conservative measures are more likely to produce a
good outcome. If the diagnosis is delayed or missed, SMA syndrome
can cause considerable morbidity and may result in potentially lifethreatening
complications.
Acknowledgments
Dept of Radiodiagnosis, Government Medical College, Nagpur.
References
Citation
Saha S, Anand A. A Rare Case of Late Presentation of Superior Mesenteric Artery Syndrome Following Kyphoscoliosis Surgery. Indian J Appl Radiol. 2020;6(1): 154.