Research Article
Cardiac CT in Coronary Artery Anomalies in Tetralogy of Fallot
Sidhu HS* and Guleria M
Department of Radiodiagnosis, ABVIMS and Dr RML Hospital, India
*Corresponding author: Sidhu HS, Department of Radiodiagnosis, ABVIMS and Dr RML Hospital, 194, Model Town Phase 3, Bathinda, Punjab, 151001, India, Mobile: 919711288355; E-mail: harsumeetsidhu@gmail.com
Copyright: © 2020 Sidhu HS, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article Information: Submission: 01/10/2020; Accepted: 02/11/2020; Published: 06/11/2020
Abstract
Objective: Cardiac CT in preoperative evaluation of coronary artery anomalies in patients with tetralogy of Fallot.
Materials and methods: Forty-six patients diagnosed with tetralogy of Fallot by echocardiography underwent cardiac CT from Jan 2017 to Jan 2020 for coronary artery evaluation. CT findings were correlated with surgical findings.
Results: Three cases (6.5%) of anomalous coronary arteries were found in our study. One case showed anomalous origin of left anterior descending artery from right sinus of Valsalva. The second case revealed single coronary artery arising from left sinus of Valsalva and bifurcating into right coronary artery and left coronary artery. The third case showed anomalous origin of right coronary artery from left sinus of Valsalva with a malignant course.
Conclusion: Cardiac CT is an accurate and non-invasive modality in preoperative evaluation of coronary artery anomalies and avoiding damage during corrective surgery in patients with tetralogy of Fallot.
Introduction
The incidence of coronary artery anomalies in patients with
tetralogy of Fallot is 2-14% [1,2]. The presence of coronary artery
anomalies leads to a change in the approach of surgical correction
in tetralogy of Fallot. Anomalous coronary artery crossing the right
ventricular outflow tract may remain undetected during the surgical
procedure due to the overlying myocardium, epicardial fat or
adhesions from previous palliative surgery [3,4]. Thus, preoperative
identification of coronary artery anomalies is recommended in these
patients to avoid damage during the corrective surgery. Coronary
artery evaluation on pediatric cardiac Computed Tomography (CT)
before surgical intervention is possible due to high temporal resolution
and Echocardiography (ECG) synchronized data acquisition [5-7].
Materials and Methods
Patient population:
Forty-six patients diagnosed with tetralogy of Fallot by
echocardiography underwent cardiac CT from Jan 2017 to Jan 2020
for preoperative evaluation. Male to female ratio was 1.7: 1 and the
age range was 21 days to 18 years with a mean of 4 years.Patient preparation:
The laterality of the aortic arch as mentioned in the
echocardiography report was useful for the site of intravenous access
in the opposite cubital fossa. A peripheral intravenous cannula, 20G
or 22G, was used according to the patient to accommodate the large
volume, high pressure contrast injection. Preparations for sedation or
anaesthesia were made as per requirement.CT and image reformatting techniques:
CT was done on 128 slice Dual Energy CT scanner (SOMATOM
Definition Flash; Siemens, Erlangen, Germany). CT data was
obtained with the following parameters: 3 mm slice thickness, 3
mm increment, 0.28 sec rotation time, 0.38 pitch and reconstructed
images of 0.6 mm slice thickness and 0.6 mm increment. A low effective radiation dose of 0.2 milliSieverts was given to the patient.
A volume of 2 ml/kg bodyweight of non-ionic iodinated contrast
agent was administered through IV cannula at a rate of 2 ml/sec via
power injector. Care bolus tracking technique was employed with the
region of interest placed within the descending thoracic aorta, at the
level of the carina and scan threshold set at 100 Hounsefield Units
(HU). Contrast saline solution of 50% dilution was utilized in bolus
chasing technique to improve contrast within the cardiac chambers.
ECG synchronized retrospective gating technique was employed for
coronary artery evaluation.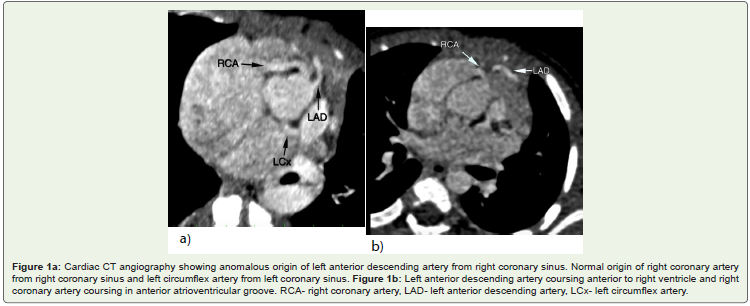
Results
Anomalous coronary arteries in 3 cases in cardiac CT are described
below.
Case 1:
Anomalous origin of left anterior descending artery from
right sinus of Valsalva was noted (Figure 1a). Its proximal segment
traversed anteriorly for a short length and then angulated towards left coursing anterior to right ventricle and further along interventricular
sulcus (Figure 1b). Left circumflex artery had normal origin from left
sinus of Valsalva and traversed posteriorly along left atrioventricular
groove. Right coronary artery had normal separate origin from right
sinus of Valsalva and traversed along anterior atrioventricular groove.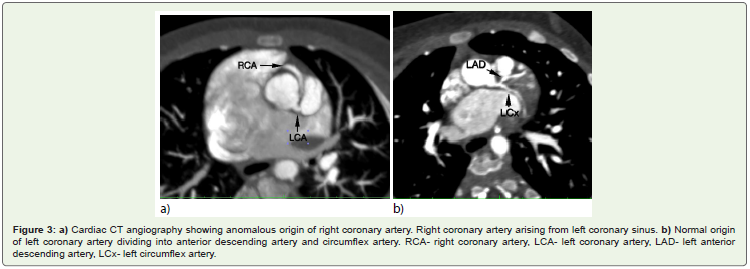
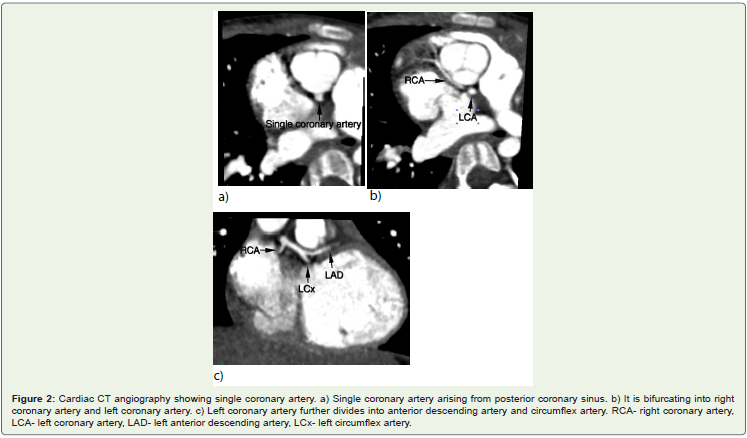
Case 2:
Single coronary artery was noted arising from left sinus of
Valsalva (Figure 2a). After a short course, the single artery bifurcated
into right coronary artery and left coronary artery (Figure 2b). Right
coronary artery traversed anteriorly between aortic root and right
atrium to reach anterior atrioventricular groove. Left coronary artery
divided into left anterior descending and left circumflex arteries
(Figure 2c). Left anterior descending artery traversed posterior to right
ventricular outflow tract for a short length and then coursed along
interventricular sulcus. Left circumflex artery traversed posteriorly
along left atrioventricular groove.Case 3:
Anomalous origin of right coronary artery from left sinus of
Valsalva was noted. Its ostioproximal segment was coursing between
ascending aorta and main pulmonary artery suggestive of malignant
course (Figure 3a). The mid and distal segments of right coronary
artery traversed along the usual anterior atrioventricular groove.
Left coronary artery had normal origin from left sinus of Valsalva
and divided into left anterior descending and left circumflex arteries
(Figure 3b). Left anterior descending artery traversed along its normal
course in interventricular sulcus and left circumflex artery traversed in
posterior atrioventricular groove.Discussion
Previous studies have shown that the incidence of coronary artery
anomalies in patients with tetralogy of Fallot is in the range of 2-14%
[1,2]. Meyer et al reported 23 cases in a study group of 926 patients with
tetralogy of Fallot having coronary artery anomalies [8]. Hurwitz et al
found 25 out of 250 patients undergoing complete repair of tetralogy
of Fallot with abnormal coronary artery [9]. Shrivastava et al studied
32 cases of coronary artery anomalies in 296 patients with tetralogy
of Fallot [10]. The incidence of total coronary artery anomalies in our study was 6.5% which was within the range of the previous reports.
Origin of the left anterior descending artery from the right
coronary artery or from a separate ostium in the right sinus of
Valsalva is the most common coronary artery anomaly associated
with tetralogy of Fallot. After its anomalous origin, the left anterior
descending artery crosses over the anterior surface of the right
ventricular outflow tract and continues in its normal course and
distribution in the interventricular sulcus. Case 1 described above
corresponds to this anomaly. Single coronary artery is the second
most common coronary anomaly in patients with tetralogy of Fallot.
The single coronary originates with equal frequency from the right
or left sinus of Valsalva. Smith reviewed three major anatomic
varieties of single coronary artery [11]: 1) a single coronary artery
following the course of either the normal right or left coronary artery
and supplying blood to the entire myocardium by its branches; 2)
a single coronary artery dividing into two major branches shortly
after its origin, each of these branches following the distribution of
the normal right and left coronary arteries; and 3) a single coronary
artery with abnormal distribution that it cannot be compared with
either the right or left coronary artery. Most of the cases reported with
tetralogy of Fallot are of the second type in which the single coronary
artery divides early in its course into the right coronary artery and left
coronary artery [12,13]. The single coronary artery described in Case
2 also corresponds to the second type as reviewed by Smith. A rare
anomaly is the origin of left circumflex artery from the right coronary
artery and crossing directly over the outflow tract, the left anterior
descending artery normally distributed and arising as the total left
coronary artery [9]. No such anomaly was seen in our patients with
tetralogy of Fallot. However, an anomalous origin of right coronary
artery from left sinus of Valsalva with malignant course was noted as
described in Case 3.
Echocardiographic analysis remains the first step in the
evaluation of patients with tetralogy of Fallot, however it may have
limitations in depicting anomalous coronary arteries. A study showed
missed coronary artery anomaly in 3 of 7 cases by echocardiography
[14]. Similarly, 1 case of missed coronary artery anomaly by
echocardiography was noted in our study. Review of literature shows
that CT is a highly accurate noninvasive modality for demonstrating coronary artery origins, their course and spatial relationships to
adjoining structures. Goo conducted a study to evaluate incidence
and diagnostic accuracy of preoperative cardiac CT for identifying
detailed coronary artery anatomy in 318 patients with tetralogy of
Fallot. Coronary artery anatomy on preoperative cardiac CT was
compared with surgical findings. Incidences of total and surgically
critical coronary artery anomalies, concordance rate between cardiac
CT and surgical findings and diagnostic accuracy of cardiac CT were
assessed. The incidences of total and surgically critical coronary
artery anomalies were 8.5% and 5.0% respectively. The concordance
rate between cardiac CT and surgical findings was 95.0% and the
diagnostic accuracy of cardiac CT was 96.9% [15]. Another study
by Vastel-Amzallag et al assessed the accuracy of preoperative
dual source CT in detecting coronary artery anomalies by using
surgical findings as the reference standard. Their study revealed
100% sensitivity and 100% specificity for detecting coronary artery
abnormalities. Major coronary artery abnormalities were found in
7% patients [14]. In addition to non invasive coronary evaluation,
cardiac CT allows accurate depiction of pulmonary artery anatomy,
major aortopulmonary collateral arteries and the aorta at the level of
diaphragm.
Chronic cyanosis with its associated rheologic changes is a
known risk factor for glomerular nephropathy. Contrast induced
nephrotoxicity thus should be an important consideration in patients
with tetralogy of Fallot. A study investigated 23 cyanotic patients for
blood viscosity and renal damage before and after administration
of non ionic contrast medium. Only one of the 23 patients showed
renal damage after contrast administration. Elevated blood viscosity
in cyanotic patients was slightly reduced by the contrast [16]. In
our study, none of the patients showed renal damage after contrast
administration.
Surgical correction of tetralogy of Fallot includes closure of
the ventricular septal defect, resection of infundibular stenosis and
pulmonary valvotomy through an incision in the right ventricular
outflow tract [17]. The standard vertical incision is given as it can be
continued through hypoplastic pulmonary annulus into the main
pulmonary artery for enlargement of these structures with a Dacron
patch. With this incision, a major coronary artery crossing the right
ventricular outflow tract can be injured easily. In most instances, the
left anterior descending artery arising from the right coronary artery
is prone to injury [18]. In such cases, a transverse or oblique incision
is given parallel to the unusual coronary artery during total correction
of tetralogy of Fallot [19]. The latter approach was followed during
total correction in Case 1, however there was no surgical concern in
Case 2 and Case 3.
The mortality rate reported in the literature is 9-30% for the repair of patients with tetralogy of Fallot and anomalous coronary artery [4,8,9,20,21]. The majority of the deaths occurred due to inadvertent division of the anomalous left anterior descending artery [4,10,20].
Other factors included inadequate resolution of the right ventricular
outflow tract obstruction and acute right ventricular aneurysmal
dilatation causing attenuation or occlusion of the overlying left
anterior descending artery. Post operative period was uneventful in
our 3 cases of tetralogy of Fallot with coronary artery anomalies.
Conclusion
Anomalous coronary arteries in patients with tetralogy of Fallot
may produce disastrous consequences during surgical correction.
Cardiac CT is an accurate and noninvasive modality for delineating
coronary artery anatomy. Echocardiography and cardiac CT have the
advantage of obviating the need for cardiac catheterization in patients
with tetralogy of Fallot.
References
Citation
Sidhu HS, Guleria M. Cardiac CT in Coronary Artery Anomalies in Tetralogy of Fallot. Indian J Appl Radiol. 2020;6(1): 152.