Case Report
Uterine Artery Pseudoaneurysm Secondary to Therapeutic Abortion Managed by Uterine Artery Embolisation
Sundeep NVK and Venkatesh M*
1Department of Radiodiagnosis, Government General Hospital and Medical College, India
2Department of Radiodiagnosis, Narayana Medical College and Hospital, India
*Corresponding author: Venkatesh M, Department of Radiodiagnosis, Narayana Medical College and Hospital, Nellore - 524 002, A.P, India
Copyright: © 2020 Sundeep NVK, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article Information: Submission: 04/02/2020; Accepted: 11/03/2020; Published: 14/03/2020
Abstract
Uterine Artery Pseudoaneurysm (UAP) is a complication of uterine curettage or surgery and is intractable to conservative treatment. Characteristic grey
scale and doppler ultrasound findings confirm the presence of pseudoaneurysm. In this case report we present a case of UAP diagnosed by ultrasound,
confirmed by angiogram and managed by embolisation.
Keywords
Uterine artery pseudoaneurysm, Post D & C complications, Persistent vaginal bleeding after therapeutic abortion, Uterine artery embolisation
Abbreviations
UAP: Uterine Artery Pseudoaneurysm
Introduction
Uterine artery Pseudoaneurysm (UAP) is a complication of
uterine curettage or surgery and should be considered when the
haemorrhage is intractable and refractory to conservative measures
[1]. Uterine artery pseudoaneurysm (UAP) is an extra luminal
collection of blood communicating with the parent vessel through
a defect in arterial wall showing characteristic Yin-an pattern on
Doppler [2,3]. It is secondary to vascular trauma, etiology includes
various pelvic surgeries and uterine procedures [4,5]. Classic
ultrasound imaging findings includes pulsating anechoic cystic
lesion [2], “yin -yan” pattern or “to and fro” phenomenon [2,5]. In
this case report we present a case of UAP diagnosed on ultrasound
and angiogram and successfully managed by selective transcatheter
embolisation
Case report
A 27 year old gravida 1, para 0, live birth 0 and abortion 1, female
was admitted to hospital with severe vaginal bleeding. Her medical
history revealed uterine curettage (D & C) for therapeutic abortion
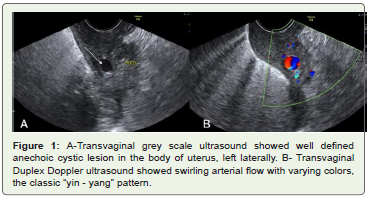
and evacuation of retained products of conception. Transvaginal
ultrasound showed well defined anechoic lesion measuring 9 x 7
mm in the body of uterus. Doppler imaging showed swirling arterial
flow with varying colours, the classic “yin - yan” pattern with narrow
neck and feeding vessel. After explaining the pros and cons of the
different treatment strategies, patient preferred minimally invasive
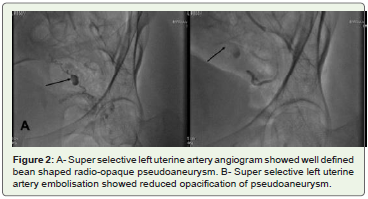
fertility preserving therapy. Patient underwent left internal iliac
artery angiogram which showed well defined bean shaped radioopaque
pseudoaneurysm arising from the left uterine artery. The
pseudoaneurysm was embolised by superselective catheterisation
of the left uterine artery. After embolisation the pseudoaneurysm
showed reduced opacification and on follow up ultrasound showed
no obvious vascularity (Figures 1 and 2).
Discussion
Uterine artery pseudoaneurysm is a rare and life threatening
vascular anomaly, secondary to injury to the artery with inadequate
sealing of the arterial wall [4]. It occurs at a rate of 0.2 % [2]. Etiology
of vascular injury includes pelvic surgeries and uterine procedures
which are caesarean section, myomectomy, hysterectomy, ovarian
cystectomy, traumatic delivery / traumatic pregnancy termination,
curettage, manual removal of placenta, vacuum extraction and
forceps delivery [4,5].
Following laceration of arterial wall, high arterial pressure gradient
causes blood to dissect into the tissue planes and forms a perfused
sac which communicates with the parent vessel [1]. In contrast with
true aneurysm, pseudo aneurysm lacks the three layered arterial wall
and usually surrounded by adjacent tissue and blood clots [5]. UAP is
prone to rupture and may be fatal, risk is proportional to the size and
intramural pressure [6].
UAP may remain asymptomatic but most of cases were reported
as immediate and significant vaginal bleeding [7]. Some instances
rupture of pseudoaneurysm involves peritoneal surface of uterus
and presents as severe hypotension and shock which indicates
intraabdominal haemorrhage [4]. Intractable haemorrhage refractory
to conservative measures may be potentially attributed to uterine
arterial injuries and UAP should be included in the differential
diagnosis, should warrant search for clinical history regarding
surgical trauma [1].
Grey scale ultrasound shows pulsatile anechoic cystic structure
in the myometrium [1,2,7]. Colour Doppler ultrasound shows swirling arterial flow with varying colours due to variable degree of
turbulence, the “yin -yan” pattern or “to and fro” phenomenon, this
can be attributed to pressure gradients between the artery and the
aneurysm cavity in systole and diastole. In systole arterial blood flows
like a jet in to the aneurysm cavity ( forward flow ) and in diastole
flow reverses ( back ward flow) in to the parent artery [1,2,5].
Angiography remains the gold standard in diagnosis of UAP [6].
Internal iliac artery angiogram shows a radio-opaque sac supplied
by one or more feeding arteries [1]. The treatment options include
hysterectomy, ligation of internal iliac artery or its branches and
uterine artery embolisation [5]. Hysterectomy should be reserved
for severe intractable hemorrhage in non reproductive age group
[5]. Ligation of arteries has its disadvantages, as the collateral supply
will establish with middle sacral, last lumbar and inferior epigastric
arteries [5]. Uterine artery embolisation is minimally invasive fertility
preserving treatment option in reproductive age group [4,5].
Embolisation of anterior division of internal iliac artery is a fast
procedure in case of emergencies and super selective embolisation of
uterine artery is an elective and time effective procedure [4].
Conclusion
Intractable haemorrhage refractory to conservative measures
may be potentially attributed to uterine arterial injuries and UAP
should be included in the differential diagnosis. Etiology includes
pelvic surgeries and uterine intervention procedures. Classic imaging
finding the “yin -yan” pattern 2 or “to and fro” phenomenon on
ultrasound. Angiography is the gold standard for diagnosis of UAP.
Tran’s catheter uterine artery embolisation is the minimally invasive
fertility preserving treatment of choice in the women of reproductive
age group.
References
Citation
Sundeep NVK, Venkatesh M. Uterine Artery Pseudoaneurysm Secondary to Therapeutic Abortion Managed by Uterine Artery Embolisation. Indian J Appl Radiol. 2020;6(1): 147.