Research Article
Risk and Survival Benefits of Percutaneous Transhepatic Biliary Drainage (PTBD) & Diagnostic Utility of Endobiliary Brush Cytology
Anand A*, Sharma D and Rathod J
Department of Radiology, Government Medical College, India
*Corresponding author: Anand A, Department of Radiology, Government Medical College, Nagpur,
Maharashtra, India, E-mail: rtanand.aa@gmail.com
Copyright: © 2020 Anand A, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article Information: Submission: 01/17/2020; Accepted: 02/03/2020; Published: 09/03/2020
Abstract
Objective: Patients of malignant biliary obstruction were prospectively & retrospectively analyzed to identify factors related to bile output and reduction
of serum bilirubin after PTBD and stenting. We also compared the survival of these patients after PTBD to investigate if biliary drainage had any impact on
the long-term survival
Materials and methods: 41 patients of malignant obstructive jaundice in whom PTBD was attempted were followed up at regular interval of 2, 6 & 12
months. Data on post-stenting complications, stent patency and patient survival were collected. Endobiliary brush cytology was performed in 18 patients
prior to dilatation and stenting.
Results: Mean age of presentation was 55 years for males and 52 years for females. Most common cause of biliary obstruction was cholangiocarcinoma.
There was significant decrease in bilirubin on postoperative day 5 with p-value less than 0.0001. Patients with dilated IHBR had better post procedural
outcome as compared to those with non-dilated IHBR. No significant association was found between extra or intra hepatic biliary dilatation and intra or
postoperative complications and long-term outcome. There was increase in postoperative survival in patients with internal drainage as compared to external
drainage. Cytology report showed malignant cells in 13 out of 14 patients.
Conclusion: PTBD is an effective procedure in malignant obstructive jaundice to reduce the bilirubin load. Long-term survival rate in case of patients
of malignant obstructive jaundice undergoing PTBD was significantly increased with 2,6 and 12 months survival rate 88.2%, 67.6% and 50%. Patients with
non-dilated system are at an increased risk of intra and postoperative bleeding as compared with the patients with dilated system. Metastasis and ascites in
case of patient with malignant obstructive jaundice are bad prognostic factors for PTBD. Endobiliary brush cytology is an important alternative to have histopathological
diagnosis in case of malignant obstructive jaundice undergoing PTBD.
Keywords
PTBD; Survival; Diagnostic; Endobiliary; Brush; Cytology
Introduction
Malignant Biliary Obstruction (MBO) is usually caused by
cholangio-carcinoma, gall bladder and pancreatic malignancies,
and metastatic lymphadenopathy and infrequently by hepatic and
advanced gastric and duodenal malignancies [1]. Where the tumors
are unresectable at diagnosis only palliative treatment is possible
to improve patient’s quality of life. The key purpose of biliary
interventions in these patients is to decompress the obstructed biliary
system. This decreases pain, jaundice and occurrence of cholangitis
by relieving the obstruction. As hepatic dysfunction is a risk factor
for major hepatic resection, biliary drainage helps in improving the
liver function prior to surgery or neo-adjuvant chemotherapy [2-4].
Surgery has been traditionally considered the treatment of choice in
patients with biliary malignancies. However a large number of these
patients are found unresectable. Among these patients reported
median survival is 3 to10 months [5]. Endoscopic stenting in patients
with low biliary obstruction is the preferred method. However, high obstructions, bilateral or multiple strictures, as well as previous upper
gastrointestinal tract surgery may render endoscopic stent placement
difficult or impossible and in such cases percutaneous technique is
preferred [6]. Percutaneous Trans-Hepatic Biliary Drainage (PTBD)
and metallic stent insertion has been practiced since the early reports
of percutaneous trans-hepatic cholangiography in the 1960s. It is
an effective preoperative risk-reducing modality and an effective
palliative procedure in patients who are not surgically drainable [7].
It is now a common procedure for the interventional radiologists
[8]. Although stenting can be performed with either Plastic Stents
(PS) or Self-Expandable Metallic Stents (SEMS), the benefit of the
latter is manifested by higher rates of successful drainage and longer
survival [9,10]. In this study we prospectively & retrospectively
analyzed the clinical and imaging characteristics of these patients in
an attempt to identify the factors related to bile output and reduction
of serum bilirubin after PTBD. In addition, we also compared the
survival of patients with different bile output and reduction rates of
bilirubin after PTBD to investigate if the short-term effectiveness of
biliary drainage had any impact on the long-term survival. Previous
studies that analyzed patient survival present outcomes that are
controversial, there is as yet no general agreement regarding either
the technique of the procedure or the selection of patients. The aim of
our study was to assess short- and long-term outcomes of malignant
biliary stricture treatment by Percutaneous Trans-Hepatic Bile Duct
Stenting (PTBS) with uncovered self-expandable metallic stents, and
to identify predictors of patient survival. It is necessary to elucidate
which features patients possess in order to ensure the maximum
possible benefits for survival. Malignant strictures of extra-hepatic
duct cannot be easily distinguished from benign strictures [11].
Biliary brush cytology can be alternative method in the evaluation of
patients with biliary tract stricture.
Material and Methods
The study was carried out prospectively on 41 patients of MBO
in whom PTBD procedure was attempted and patients were followed
up at regular interval of 2, 6 & 12 months. Duration of study was
2 years. Ethical clearance was obtained from ethical committee
of the institution. Well informed consent was obtained in all cases
after explaining about the procedure and its complications in detail.
All patients with surgical obstructive jaundice were assessed with
multiphase Contrast Enhanced Computed Tomography (CECT)
and Magnetic Resonance Cholangio Pancreatography (MRCP) prior
to percutaneous management, for identifying the level and cause of
obstruction and defining the extent of the disease. Ultrasonography
was done as a screening procedure prior to percutaneous
intervention to assess biliary dilatation, presence of ascites, volume
of the liver lobes/segments and patency of biliary confluence
(primary and secondary) as this decided the approach used and lobe
to be drained. Patient’s coagulation profile was checked before the
procedure to avoid bleeding complications. If Prothrombin Time
and International Normalized Ratio (PT/INR) values were deranged,
vitamin K injection was given for three days and the procedure was
done after normalization. In case of emergencies where the patient
had cholangitis with risk of septicaemia, if PT/INR was deranged,
fresh frozen plasma was given before and during the procedure.
The procedure was usually performed under local anesthesia in the
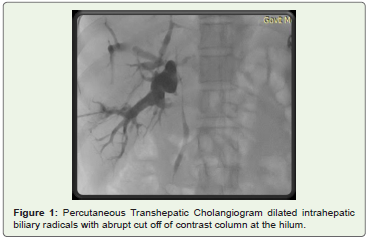
presence of anesthetist. The segmental duct was punctured by spinal
needle and percutaneous cholangiogram was performed slowly to
define the biliary anatomy and type of obstruction (Figure 1). Later
on the radicals were punctured with 18 G Chiba needle or 18G
spinal needle, under fluoroscopy /ultrasonography guidance. Once
there was backflow of bile, a 0.032/0.035 inch soft “J” tip guide wire
is passed through the needle, which was then exchanged for a 5F
or 6F dilator followed by removal of the guide-wire. Subsequently,
the dilator was exchanged for 7F Angiosheath or an angled tip
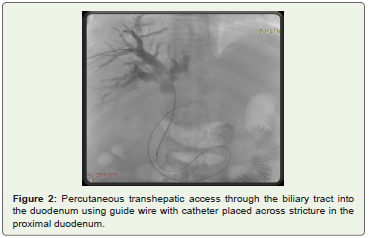
angiographic catheter over the wire. When the catheter tip was at the
site of obstruction, the soft hydrophilic guidewire was manipulated to
cross the stricture. Once the wire was across the stricture, the catheter
was pushed over the wire into the duodenum (Figure 2). The soft wire
was then replaced by Ultra Stiff Amplatz guidewire over which the
tract and stricture was dilated. Then, an 8F/8.5F internal-external
drainage catheter was positioned across the stricture and the position
was confirmed with contrast injection. In patients where initial
attempt to cross the stricture failed, an external drainage catheter
was left with tip proximal to the obstruction and internalization
was attempted after a gap of two-four days. This two-step procedure
helped in reduction of inflammation and edema and enhanced the
likelihood of negotiating the obstruction. For strictures distal to the
hilum, with patent primary biliary confluence, single drainage was
sufficient. Drainage of single or both systems was done when the
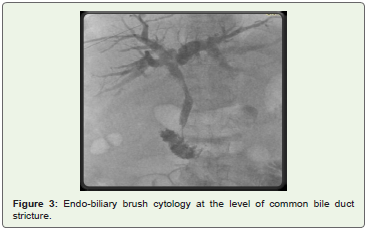
primary biliary confluence was completely occluded. Endobiliary
Double Lumen brush was used for sampling prior to dilatation and
stenting by agitating the brush in between the stricturous segment
(Figure 3). Samples were then taken on slides and sent to cytology
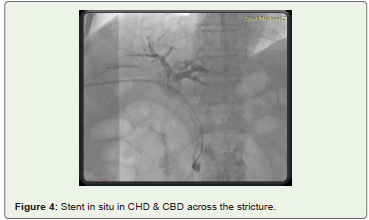
department. Once the obstruction was traversed, stenting was done
in the same sitting to reduce the incidence of procedure related
complications. Self expandable metallic stents (Zilver Flex by Cook
medical services/ WalllFlex metallic stent by Boston) were used
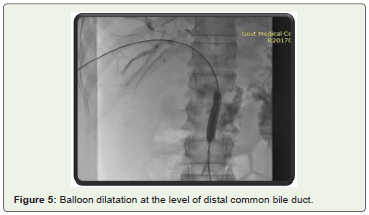
(Figure 4). The stricture was dilated with plastic dilators, if necessary,
so that the stent apparatus could be passed. The metallic stents have
thermal memory and expand to their maximum width when they
reach the body temperature, this usually occurs in 24-48 hr. If the
expansion was not adequate after 48 hr, dilatation of the stent with
balloon catheter was done for successful drainage (Figure 5). Data
on post-stenting complications, stent patency and patient survival
were collected retrospectively from patient’s medical records & postoperative CT scans taken before patient was discharged. Further
follow up of patients was taken telephonically at regular interval of 2
months, 6 months and 1 year. Continuous variable were presented
as mean +SD. Categorical variables were expressed in frequency and
percentage. Paired T test was performed to compare preoperative and
postoperative bilirubin levels. Categorical variables were compared
by performing chi-square test. For small numbers, fisher exact test
was applied wherever required. All the test were two sided. p- <0.05
was considered as statistically significant. Statistical software Stata
version 14.0 was used for data analysis.
Results
Most of the population in this study was above the age of 40 years
with maximum patients in age group of 51-60 years. Mean age of
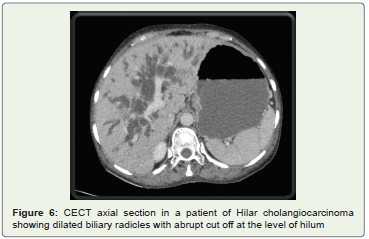
presentation was 55 years for males and 52 years for females. Most
common cause of biliary obstruction on preoperative imaging in
our study was cholangiocarcinoma followed by carcinoma head of
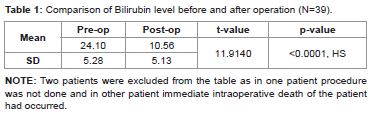
pancreas (Figure 6). Mean bilirubin level of the patient at the time of
presentation was 24.10 mg/dl. Almost all of the patients experienced
decrease in clinical jaundice and associated symptoms (e.g. pruritus)
after PTBD with mean postoperative bilirubin value being 10.5 mg/
dl. There was statistically significant decrease in the postoperative
bilirubin value done at postoperative day 5 with p-value less than
0.0001, which is highly significant (Table 1). As most of the patients
presented late and in advanced stage, severe Intrahepatic Biliary
Radical (IHBR) dilatation (>2 mm) was seen in 32 patients. In
9 patients IHBR was found to be non dilated. These findings were
correlated with the intra and postprocedural complication (e.g.
Bleeding and sepsis). It was found that patients with dilated IHBR
had better post procedural outcome as compared to the patients with
non-dilated IHBR. This can be correlated with difficulty in puncture
of the biliary radical in non-dilated biliary system with more chances
of vascular injury by multiple punctures. Out of the 32 patients with
dilated IHBR 29 (90.6%) patients survived till 2 months, 20 (62.5%) patients survived by 6 months and 17 (53.1%) patients had survival
of more than 1 year. Out of the 9 patients with non-dilated system
2 patients (22.2%) had intraoperative or postoperative bleeding. No
significant association was found between the Extrahepatic Biliary
Radical (EHBR) dilatation and intra or postoperative complications
& postoperative long-term outcome. Out of 41 patients, 22(53.6%)
patients had hilar obstruction, which was correlated with the postoperative
outcome. There was significant improvement in longterm
survival in patients with hilar obstruction as compared to
patients without hilar obstruction with post operative 2,6 and
12 months survival rate of 86%, 63% and 45% respectively. Level
of obstruction was also correlated with intraoperative and postoperative
complications. Out of 22 patients with hilar obstruction
2 patients had severe bleeding and 1 patient landed in sepsis in
postoperative period. Out of 22 patients with infrahilar obstruction
2(9.5%) patients had severe bleeding in intra-postoperative period
and 1 patient had sepsis in postoperative period. 15 (36.5%) patients
had metastatic lesions (in the liver and/or lymph nodes). These
patient’s post operative outcomes were compared with those of
patient’s without metastatic lesions. One patient with metastasis was
excluded from the postoperative outcomes because of failure of the
procedure in this patient. There was significant decline in the survival
of patients with metastasis with postoperative long-term survival
at 2,6 and 12 months of 85%, 46.6% and 33.3% as compared with
that of 88%, 72% and 56% in patients without metastasis. However
no statistical significance was demonstrable. So metastasis in case of
patient with MBO is bad prognostic factor for PTBD patients. Out
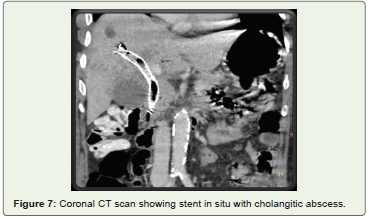
of 10 patients with gross ascites 4 patients (36.4%) had episodes of
bleeding intra or postoperative period. 1 patient (9.1%) landed in
severe sepsis in postoperative period (Figure 7). There was significant
statistical correlation between ascites and intra or post operative
bleeding. One patient was excluded from the calculation, as PTBD
was not performed even after repeated attempts. In 6 (14.6%) cases
it was not possible to put a self-expandable metallic stent (internal
drainage) due to technical difficulty in crossing the stricture and due
to non-affordability for the stents. In these patients PTBD was done
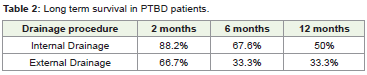
with external drainage catheter. Long-term survival in these patients
with external drainage in situ at 2,6 and 12 months was 66.7%, 33.3%
and 33.3% respectively. Internal drainage was possible in 34(82.9%)
patients. In these patients there was statistically significant increase in
survival with 2,6 and 12 months survival rate 88.2%, 67.6% and 50%.
There was increase in postoperative survival in patients with internal
drainage as compared to the external drainage (Table 2). However
this was not significant statistically. This can be due to less number
of patients who had undergone external drainage only. There were
incidents of displaced external drainage catheter, accidental removal
of external catheter, pericatheter leak & abdominal discomfort etc.
with the external drainage catheter. Out of 41 patients 39 patients
were followed up for the post PTBD serum potassium levels at post
operative Day 3. There was decrease in serum potassium levels below
3.5 in 9 (23.7%) patients. However there was no significant increase in
the postoperative mortality noted in these patients. Out of 41 patients
with MBO Endobiliary Brush Cytology (EBBC) was performed in 18
patients out of which in 14 patients (77.7%) cytology report showed
sample adequate for reporting. In 4 patients sample was reported as
inadequate. Out of 14 patients with adequate samples 13 patients
were reported to have malignant cells in the stained smears, however
in 1 patient only fibrotic tissue was reported with none of the slides
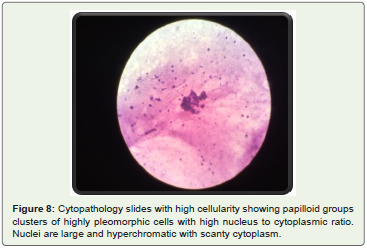
showing malignant cells. Out of 22 cases of hilar obstruction EBBC
was performed in 10 patients out of which 8(80%) cases were reported
to be adequate samples. Out of these 8 samples collected 7 samples
were positive for malignant cells (Figure 8). Similarly in 22 cases of
infrahilar obstruction EBBC was performed in 9 patients out of which
6 (67%) samples were reported to be adequate samples. Out of these 6
samples all 6 were reported to be positive for malignant cells.
Discussion
In 14th Aichi International Cancer Symposium on Pancreatobiliary
Cancer Update -Prevention, Diagnosis and Treatment by Palepu
Jagannath et al., it was observed that most of the Pancreatobiliary
tract carcinomas are observed above the age group of 50 years [12].
Our study was in concordance with this as most of the patients in
our study presented after the age of 50 years. In this study 67% of the
population were males. These findings are consistent with the study of
Zhang et al on clinical outcomes and prediction of survival following
percutaneous biliary drainage for MBO in which most of the study population was male [13]. In our study both males and females
were having nearly same age of presentation with males presenting
slightly late age of presentation. This was also in concordance with
the study of Katabi et al. and in most of the other previous studies in
which incidence of MBO is more common in males than in females
with nearly same age of presentation [14]. This may be attributable
to the number of risk factors like alcohol, smoking etc. which are
more common in males and also to the awareness of people about
the disease. Most of the patient experienced statistically significant
decrease in the level of total bilirubin. This was consistent with the
study of Tuqan et al. in which significant decrease in post operative
bilirubin was shown [15]. The technical success of PTBD in terms of
internal or external drainage in 40 patients out of 41 (97.5%) was in
concordance with the study of Pranculis et al. who reported success
rate of 95.9% [16]. Out of 41 patients, 32 (78%) showed dilatation
of IHBR and there was favorable 2, 6 & 12 months postoperative
survival in them. However in non-dilated system there was increased
chances of bleeding and postoperative mortality as compared to
that with the dilated IHBR. This is in concordance with the study of
Weber et al. concluding non-dilated intrahepatic bile ducts showed
a higher risk for procedure related complications [17]. In our study
we also compared the level of obstruction (hilar and infra-hilar) with
the postoperative complications and long-term survival. There was
no statistically significant improvement in long-term survival of the
patients with hilar obstruction. Similarly no significant correlation
was found between the level of obstruction and postoperative
complications. There was significant decline in the survival of
the patients with metastasis. Similarly study done by Li et al also
concluded metastasis as one of the independent risk factor in case
of patients undergoing PTBD in MBO [18]. Out of 41 patients in 9
patient with gross ascites (defined as patients with fluid in perihepatic
region) there was significant reduction in the survival, which was also
proven statistically (p-value-0.018). These findings were supported by
studies done by Li et al and Tuqan et al. [15,18]. Long term survival
in patients with external drainage in situ at 2, 6 and 12 months
was 66.7%, 33.3% and 33.3% respectively. However no statistical
significance was demonstrable (p value <0.407). In 33 patients of
internal drainage done there was statistically significant increase in
survival with 2, 6 and 12 months survival rate 88.2%, 67.6% and 50%.
Double stents were placed in 14 patients and single self-expandable
stent was placed in the 19 patients with infrahilar obstruction. This
is in concordance with the Pranculis et al. in which post procedural
30 days mortality rate was 15.3% [16]. Our study also depicts the
same result with post procedural survival rate at 2 months of 88.2%.
This suggests the need of another comparative prospective study
to compare internal and external drainage in terms of long-term
survival. In 9 patients there was decrease in serum potassium levels
below 3.5 at post operative day 3. However there was no significant
increase in the postoperative mortality noted in these patients. The
study was biased because of supplementation of serum potassium
orally and intravenously hence no significant correlation between
postoperative serum potassium level and postoperative mortality can
be predicted from this study. Parıldar et al. studied effects of PTBD
on renal function in patients with obstructive jaundice using the
estimated glomerular filtration rate (eGFR) and evaluated the factors
associated with renal dysfunction [19]. They observed eGFR was <60-
mL/min/1.73 m2 before PTBD in 27 patients (25%) and increased
significantly 30 days after PTBD. Conclusion of the study was that
obstructive jaundice is associated with renal dysfunction, and serum
direct bilirubin is a significant predictor of renal function. However
this can’t be correlated with our study. Endobiliary brush cytology
is an important alternative to have histo-pathological diagnosis in
case of MBO undergoing PTBD. Endobiliary brush cytology was
performed in 18 patients out of which in 14 patients (77.7%) cytology
report showed sample adequate for reporting. Out of these 13
patients was reported to have malignant cells in the stained smears,
however in 1 patient only fibrotic tissue was reported with none of
the slides showing malignant cells. This was in concordance with
the study of Xing et al in which percutaneous Trans-Hepatic Biliary
Cytology (PTBC) was done during the procedure in 58 patients with
obstructive jaundice [11]. Their results indicated that PTBC was very
easy to manipulate and had a high sensitivity. Similarly in our study
there was no difficulty in manipulating the procedure for EBCC and
there was no increase in any intra operative complications noted.
However sensitivity and specificity of this test cannot be determined
due to lack definitive gold standard test.
Conclusion
Percutaneous Transhepatic Biliary Drainage is an effective
procedure in malignant obstructive jaundice to reduce the bilirubin
load. Long-term survival rate in case of patients of malignant
obstructive jaundice undergoing PTBD was significantly increased
with 2, 6 and 12 months survival rate 88.2%, 67.6% and 50%
respectively. Patients with non-dilated system showed an increased
risk of intra and postoperative bleeding as compared with the patients
with dilated system. Metastasis and ascites were bad prognostic factors
for PTBD. Endobiliary brush cytology is very easy to manipulate and
is an important alternative for histo-pathological diagnosis.
References
Citation
Anand A, Sharma D, Rathod J. Risk and Survival Benefits of Percutaneous Transhepatic Biliary Drainage (PTBD) & Diagnostic Utility of Endobiliary Brush Cytology. Indian J Appl Radiol. 2020;6(1): 146.