Case Report
A rare Congenital Left Lung Hypoplasia with Absent Left Pulmonary Artery and Right-Sided Aortic Arch: a Dilemma in work Fitness Radiograph
Eldeeb AM*, Shukri K, Moustafa A and Al-Kuwari M
Department of Clinical Imaging, Hamad Medical Corporation (HMC), Qatar
*Corresponding author: Eldeeb AM, Department of Clinical Imaging - Communicable Disease Center (CDC), Hamad Medical Corporation (HMC), Doha, Qatar, Email: AEldeeb@hamad.qa
Copyright: © 2020 Eldeeb AM, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article Information: Submission: 02/12/2020; Accepted: 29/01/2020; Published: 03/02/2020
Abstract
Purpose: The purpose of this study is to describe congenital anomaly of unilateral absence of pulmonary artery (UAPA) which lead to a dilemma in health clearance certificate.
Material and Methods: Two consequent cases were included in the current study presented to the Communicable Disease Center (CDC) referring from Medical Commission with abnormal chest x-ray for further evaluation. Plain x-ray well studied and followed by CT scan with contrast with post processing were done.
Pictorial review: UAPA is considered rare of entity constituting a ratio of 1: 200,000, however it should be included in the differential diagnosis and containment by CT scan and post processing technique.
Conclusion: CT scan and post processing technique should be carried out to confirm the suspicious of UAPA which should be included as a differential
diagnosis.
Keywords
Unilateral absence of pulmonary artery (UAPA); Pulmonary hypertension (PHT); Tetralogy of Fallot (TOF); Computer tomography scan (CT scan); Volume rendering techniques (VRT); Maximum intensity projection (MIP); Multiplanar projections reconstruction (MPR); Tissue transparent projection (TTP)
Introduction
Congenital anomalies of the respiratory system include wide
range of varieties. It might include lung hypoplasia or aplasia and
a wide range of associated vascular and cardiovascular anomalies.
Unilateral absence of pulmonary artery (UAPA) is extremely rare
pathological entity, with its prevalence around 1:200,000 young
individual adults [1,3,4]. It has no sex prevalence, with equal male to
female ratio. It might be associated with cardiovascular abnormalities
such as tetralogy of Fallot (TOF), septal defect arterial or ventricular
as associated congenital malformation in 0.34% of the congenital
heart disease, yet it can present as isolated entity [17].
Usually the patient with sole UAPA is asymptomatic until
adulthood. However associated symptoms may include dyspnea,
chest pain, hemoptysis and recurrent attacks of the chest infection
which can supervene.
The routine investigation including chest x-ray, echocardiography
may suggest the diagnosis of absent pulmonary artery, but
conformation is required by CT scan or magnetic resonance
angiography (MRA). An early diagnosis of UAPA and appreciate
intervention may significantly improve the outcome. It might be a
cause of diagnostic dilemma during radiography for work fitness
purpose or residence permit.
Case Report
The current study includes two patients, a 27 years old male
and a 26 years old female, both came from Indian subcontinent.
The patients were referred from Medical Commission Center to the
Communicable Disease Center in Doha with abnormal Chest X-ray
findings in order obtain health fitness report clearance for working
permit, especially to rule out TB. Both patients were clinically
and physically healthy and fit with no positive medical or surgical
history. The patients had no history of parent’s consanguinity or
other siblings’ congenital anomalies, no history of drug intake by
their mothers during pregnancy period, or any abnormal incidental
radiation exposure, normal vaginal delivery for both of them. Both
patients with average body weight and height, normal vital signs,
normal oral temperature, peripheral pulse, respiratory rate, blood
pressure and oxygen saturation (SPO2). No history of any allergy,
night sweating or weight loss. On physical examination there
were: normal breath sound, normal heart sounds, no skin rash, no
palpable lymphadenopathy, soft lax abdomen, no organomegaly, no
neurological deficit. Unremarkable CBC, QUANTIFERON test is
negative and TB PCR was negative.
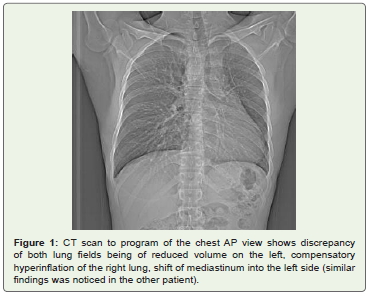
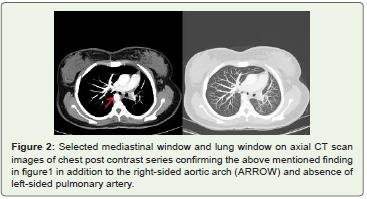
A multidetector CT scan (MDCT) of the chest before and after
IV contrast administration of non-ionic contrast media was done, it
revealed reduced volume of the left lung/hypoplasia, absence of the
left pulmonary artery/agenesis with otherwise normal caliber and
opacification of the main pulmonary trunk and the right pulmonary
artery and its segmental and its subsegmental branches, the aortic
arch was abnormally located on the right side with slightly higher
position of the left diaphragmatic copula (Figure 1,2).
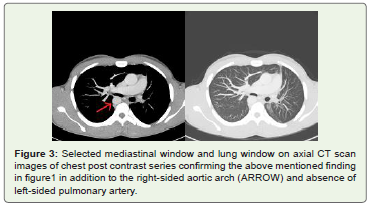
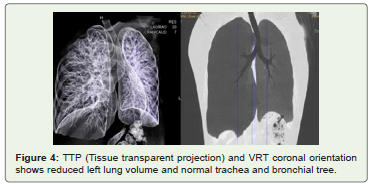
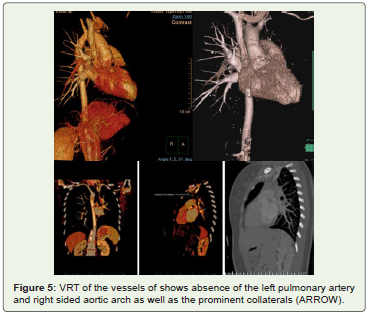
Furthermore, there was evidence of arterial collaterals on the left
chest wall as well as prominence of the left internal mammary artery.
The findings are clearly visualized with the use of volume rendering
techniques images (VRT), maximum intensity projection images
there (MIP) as well as the reconstruction in multiplanar projections
(MPR) (Figure 3-5).
Discussion
The unilateral absence of pulmonary artery (UAPA) is a rare
vascular malformation discovered and it was published for the first
time at the year 1868 [1]. The UAPA can occur in both sexes equally,
the mean age of UAPA at presentation is mostly at the age of 14 years
[1,2]. In our cases there was slightly delayed diagnosis up to 26 years/27
years. The UAPA statistically founded isolated between1:200,000 to 1:
300,000 [1,3,4]. Right-sided UAPA is more predominant and appear
about twice than the left side, however left-sided UAPA is found to be
less frequent [1,3]. It can be embryologically explained as a result of
failure in the connection of the sixth aortic arch with the pulmonary
trunk [5,6]. There are multiple factors that may play a role in
pulmonary artery (PA) agenesis with pulmonary hypoplasia among
the etiology such as chromosomal defect, exposure to intrauterine
infection, Vitamin A deficiency and some environmental factors
[1,2]. However, UAPA associated with regression of the blood supply
to the affected lung causing a result of paucity of vascular markings,
lung to appear hypoplastic with reduced volume. Most of the patients
presented in the literature were found asymptomatic, which is similar
to our cases. Up to 30% of them may stay clear and asymptomatic
until adulthood [1,2]. However, some symptoms can be occurring
such as exercise intolerance, recurrent cough or recurrent chest pain
[7-11]. The pulmonary hypertension (PHT) mainly discovered at the
infant age in those cases of left side UAPA, and those patients are
mostly surviving until adulthood [7,8]. Life threatening complication
such as hemoptysis due to excessive development of collateral can
be presented in some cases [7,8,12,13]. Bronchiectases may appear
as sequel of recurrent pulmonary infection, they were not present in
our cases [8,9]. Diagnosis of UAPA can be suspected from plain CXR
with such findings as lung volume reduction, crowding of the ribs,
ipsilateral elevation of the diaphragm, contralateral compensatory
hyperinflation, absence of the pulmonary artery shadow on the
affected side, slight paucity of vascular markings [8,14]. CT scan
of the chest with IV contrast and MRI plays an important role in
confirming the diagnosis of UAPA, which gives accurate anatomic
details, vascular collaterals or any cardiac anomaly. Pulmonary
angiography is considered as a gold stranded procedure for accurate
diagnosis of UAPA. However, it is an invasive radiological procedure
which is mostly advices for those patients who need bronchial
arterial embolization as a treatment of haemoptysis. [8,9,14]. Trans
thoracic echocardiogram has an important role in most of associated
cardiac anomalies and for assessment of pulmonary hypertension
(PHT) [12]. While the perfusion-ventilation scan (V/Q) is used to
evaluate the pulmonary activity in the normal lung and in the affected
one. The difference in activity in bilateral lung fields considered as
important part in confirming the diagnosis [12]. The patients who
were proved to have UAPA, need further evaluation including
routine echocardiography for monitoring of asymptomatic patients
to rule out pulmonary hypertension as a complication [14,15]. This
could be usually managed with pulmonary hypertension vasodilator
therapy [7,14,16]. Patients with congenital heart defects associated
with UAPA need palliative surgical intervention as pulmonary artery
shunt, transluminal balloon pulmonary valvuloplasty or palliative
reconstruction of the right ventricular outflow tract [17,18]. Our
two cases were referred to rule out tuberculosis infection, which was excluded based on x-ray and CT. The chest x-ray and CT chest
revealed congenital absence of the left pulmonary artery, left lung
hypoplasia and right sided aortic arch. Bronchoscopy done for
one patient and result was negative for TB. Medical examination
including chest radiography is essential to get significant of medical
clearance and accordingly the process of residency can be continued.
Any suspicious or any abnormal findings result in a delay of the
process and it is considered as a dilemma for work fitness it needs
further workup for deceleration.
Conclusion
Agenesis of the left pulmonary artery is a rare entity and adult
patients are often asymptomatic. Imaging plays a major role to
confirm diagnosis and detecting the associated findings in heart
and lungs. Those patients with chest x-ray usually show unilateral
relatively small left hemi thorax. The deferential diagnosis (UAPA)
should be considered and kept in mind and subsequently the mystery
and clinical diagnostic challenge situation can be solved. On the other
hand, early diagnosis help in avoidance of serious complications, like
haemoptysis that might supervene and work fitness. Despite of being
a rare entity (UAPA), however it should be kept in mind, including
in differential diagnosis and confirm by cross-sectional images (CT
scan).
References
Citation
Eldeeb AM, Shukri K, Moustafa A, Al-Kuwari M. A rare Congenital Left Lung Hypoplasia with Absent Left Pulmonary Artery and Right-Sided Aortic Arch: a Dilemma in work Fitness Radiograph. Indian J Appl Radiol. 2020;6(1): 145.