Case Report
Endovascular Management of a Case of Large Intraparenchymal and Subcapsular Hematoma of the Liver with Hepatic Arterioportal Shunt
Yugandhar S1*, Thirunavukkarasu S2, Srinivas MG3, Anusha G4 and Amitha Vikrama KS55
1Department of Radiology, Narayana Medical College and Hospital, India
2Department of Surgical Gastroenterology, Narayana Medical College, India
3Department of Medical Gastroenterology, Narayana Medical College, India
4Department of Radiology, Narayana Medical College, India
5Department of Radiology, Sakra World hospital, India
*Corresponding author: Yugandhar S, Assistant Professor, Department of radiology, Narayana Medical college and hospital, Nellore, Andhra Pradesh, India; E-mail: yugu.samireddypalle@gmail.com
Copyright: © 2019 Yugandhar S, et al. This is an open access article distributed under the Creative Commons Attribution License,
which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article Information: Submission: 29/09/2019; Accepted: 29/11/2019; Published: 02/12/2019
Case Report
A 19 year old male came with complaints of severe
right hypochondriac pain since 2 days. There was no
history of trauma. He had past history of two attacks of
acute pancreatitis for which he underwent conservative
management in outside hospital. The last attack of
pancreatitis was 4 months back. On examination at
admission, there was mild tenderness in the hypochondriac
region. His vitals were stable.
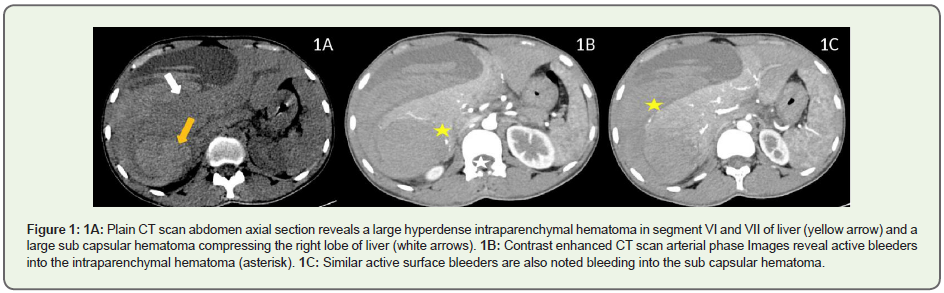
Ultrasound abdomen revealed a large intraparenchymal
hematoma measuring 8 x 7 x 6 cm in segment VI and
VII of liver which has ruptured with resultant massive
sub capsular hematoma compressing the right lobe of
liver parenchyma, which measured 14 x 12 x 11 cm. CT
angiogram was advised for further evaluation which
confirmed the ultrasound findings. There was marked
extrinsic compression of right lobe of liver. There were, in
addition, multiple small bleeders into the intraparenchymal
hematoma as well as extensive surface bleeders on the raw
surface of right lobe of liver, most of which appear to arise
from the peripheral portal vein radicles. The right anterior
branch of the portal vein was enhancing in the arterial
phase with wedge shaped transient hepatic parenchymal enhancement during the arterial phase, suggesting the
presence of arterioportal shunt (Figure 1).
His Liver function tests and other blood parameters
were normal. As the patient was clinically stable except for
pain, it was decided to manage conservatively. However,
during the hospital stay, there was a rapid and significant
drop in the haemoglobin from 13 gm/dl on the day of
admission to 6gm/dl in 36 hours. His pain worsened and
there was tachycardia. So, it was decided to evaluate him
with hepatic angiogram to look for abnormal bleeders.
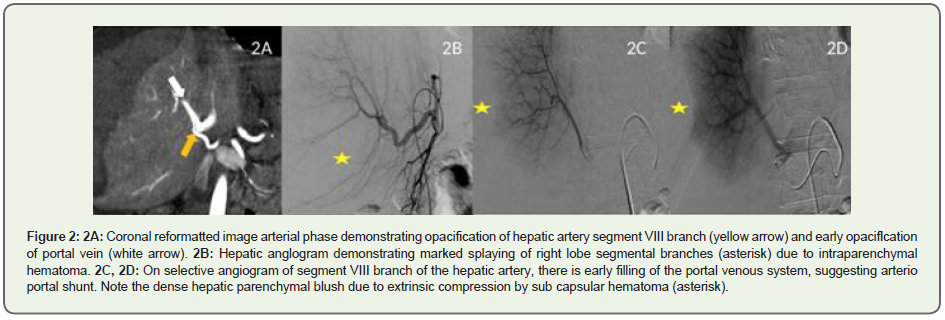
Selective angiogram of segment VI branch of hepatic artery
revealed abnormal vascularity which was embolized by
75 - 150 micron size PVA (Polyvinyl alcohol) particles.
Segment VIII branch angiogram revealed an arterioportal
shunt. Rest of the segmental arteries were unremarkable.
Since the surface bleeders were from the peripheral portal
vein radicles, it was decided to selectively embolize the
arterioportal shunt to reduce the pressure in the portal
vein system (Figure 2).
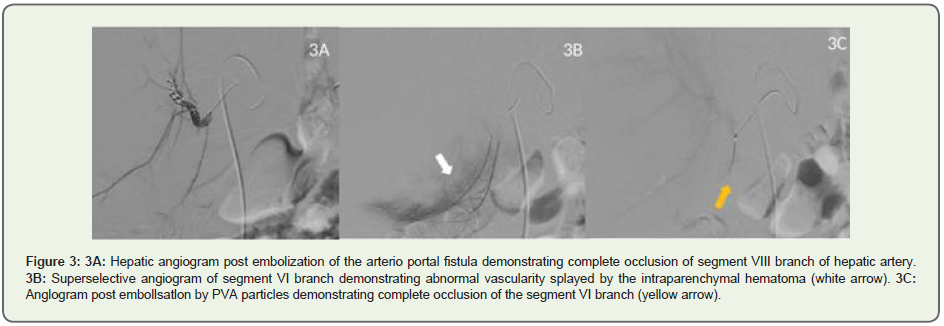
Two 018 inch coils, 3 mm x 14 cm and 3 mm x 7 cm
(Micronester coils, Cook)was placed in the segment VIII
branch of hepatic artery and the arterioportal shunt
was embolized. Post procedure, there was significant
resolution in the right hypochondriac pain within 6 hours.
There was no further drop in haemoglobin. His liver
enzymes, especially the transaminases were transiently
elevated (AST - 1200 U/L and ALT - 1300 U/L) on the
second day post procedure, but became normal in next
48 hours. Patient was discharged in stable condition on
the 5th day post procedure. His haemoglobin at the time
of discharge was 6.7 gm/dl. Follow up USG after 10 days
revealed organising sub-capsular hematoma which was
mildly regressed in size and extent (Figure 3).
Discussion
Hepatic arterioportal shunts are a well-known entity.
These can be broadly classified into tumorous and nontumorous
arterio portal shunts. These can be usually seen
in hepatocellular carcinoma. Small peripheral arterioportal
shunts are well known in cirrhosis. Large direct fistulas
can be seen in penetrating injuries of liver. Some of the
arterio portal shunts can be seen in portal vein and hepatic
vein thrombosis and also in marked extrinsic compression
of liver as in our case. The proposed mechanism for this
is increased sinusoidal pressure leading to shunting of blood from the hepatic arterioles to portal vein radicles
in the liver sinusoids, leading to opacification of the portal
vein [1]. Large direct arterioportal fistulas can be seen
in congenital vascular malformations and can also be
iatrogenic post liver biopsy [2]. Large arterioportal shunts
can be symptomatic and can result in portal hypertension
and gastric variceal haemorrhage or ascites [2,3]. In our
case, there was also a large intraparenchymal hematoma
apart from sub capsular hematoma, which can be either
due to concealed history of trauma or secondary to bleed
within primary hepatic tumour like hepatic adenoma
or hemangioma. Such cases are reported in literature,
especially in HELLP (Hemolysis, elevated liver enzymes
and low platelets) syndrome in patients with preeclampsia
.Most of these cases are usually conservatively managed, if
the clinical and lab parameters are within normal range.
Sometimes, patients present with intra peritoneal rupture
and shock [4]. We had to intervene in this case as there was
significant drop in Haemoglobin in 36 hours of admission
with tachycardia. Such hematomas are also reported in
post liver transplant cases were hepatic angiogram was
done in necessary cases to look for source of bleed. Hepatic
arterioportal shunts can be seen in such conditions, which
were embolised [5].
Due to shearing away of the liver capsule from raw
surface of liver, extensive surface bleeders are usually seen
in such rapidly expanding sub-capsular hematomas. In our
case, most of these surface bleeders appear to arise from
the peripheral portal vein radicles in CT angiogram and
the presence of arterioportal shunt in hepatic angiogram
is an indirect indicator of active haemorrhage [5]. The
shunts could have made these surface bleeders as high
pressure bleeders as the portal vein pressures would have increased due to shunting. These surface bleeders
cannot be embolized. As there was Haemoglobin drop and
early signs of hypotension, embolization of arterioportal
fistula was considered to stop arterial haemorrhage and
also reduce the pressure of surface bleeders from portal
radicles which could help in spontaneous haemostasis.
Various embolization agents can be used to embolize
the hepatic arterioportal shunts like detachable balloons,
coils and microspheres [6]. The transient increase in the
liver enzymes can be explained by marked parenchymal
compression. These abnormal parameters, however, were
normalised in 48 hours post procedure. Still conservative
management has to be initially tried in these cases if the
patient is clinically stable. If there is continuing drop
in haemoglobin and signs of hypotension/shock, the
causative factors have to be evaluated and an attempt for
embolization should be done.
References
Citation
Yugandhar S, Thirunavukkarasu S, Srinivas MG, Anusha G, Amitha Vikrama KS. Endovascular Management of a Case of Large Intraparenchymal and Subcapsular Hematoma of the Liver with Hepatic Arterioportal Shunt. Indian J Appl Radiol. 2019;5(1): 143.