Research Article
Role of High Resolution Ultrasonography Evaluation of Thyroid Nodules and Pathological Correlation
Penaka H1, Venkatesh M1* and Manjunatha YC2
1Department of radiodiagnosis, Narayana medical college & hospital, India
2Consultant Radiologist Sree chowdeswri, Multispeciality Hospital, Kolar, Karnataka, India
*Corresponding author: Venkatesh M, Assistant Professor, Department of radiodiagnosis, Narayana medical
college & hospital, Nellore-524 002, A.P, India
Copyright: © 2019 Penaka H, et al. This is an open access article distributed under the Creative Commons Attribution
License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is
properly cited.
Abstract
Aims and objectives: To identify morphologic patterns on High Resolution Sonography (HRS) those are predictive of benign and malignant nodules and to evaluate the efficacy of histopathology and HRS in differentiating benign and malignant nodules.
Materials and methods: Over a period of 18months, 50 patients referred for USG of the thyroid to R.L. Jalappa Hospital and Research Centre, Tamaka,
Kolar, Karnataka who were diagnosed clinically with solitary thyroid nodule. Thyroid sonographic findings relevant to benign or malignant nodules were
recorded and these findings were compared with histopathology reports of the thyroidectomy specimen.
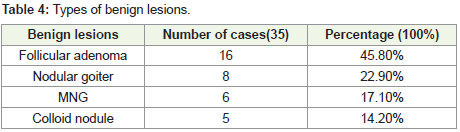
Results: Out of 50 cases of solitary thyroid nodules, 35(70%) cases were benign and 15(30%) were malignant. Among benign lesions, adenomas were
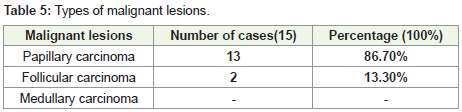
the most commonest group comprising 45.8%, followed by nodular goiter 22.9%. Among malignant, papillary carcinomas were the most commonest group
86.7%, followed by follicular carcinoma 13.3%. Majority of the patients are in the age group of 31-40 years. Among malignant lesions, papillary carcinoma was
the most common and medullary was the least common type. Follicular carcinoma was seen in 2(13.3%) cases among malignant lesions. Out of 50 cases of
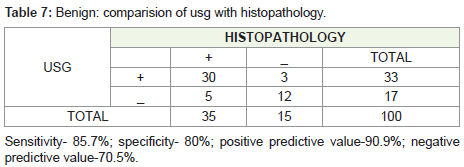
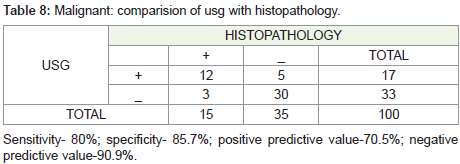
solitary thyroid nodules evaluated at USG, 33 were diagnosed to be benign, 17 were malignant, after histopathological evaluation, 35 out of 50 cases were
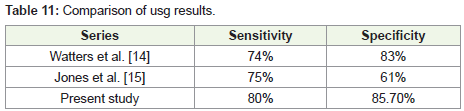
found to be benign and 15 were malignant. Ultrasound is a safe, fairly accurate investigation to differentiate benign from malignant etiology with sensitivity of
85.7 % and specificity of 80 %. USG proved to be a more sensitive modality to differentiate benign from malignant lesions.
Conclusion: Thyroid nodules were common in the females of age group 31-45 years. Ultrasound is a safe, fairly accurate investigation to differentiate
benign from malignant etiology with sensitivity of 80% and specificity of 85.7%. Ultrasound features of thyroid nodules are useful to distinguish patients with
clinically significant thyroid nodules from those within nocuous nodules despite the overlap of findings
Keywords
Solitary thyroid nodule; High resolution sonography; Histopathology; Sensitivity; Specificity
Introduction
Thyroid nodules are a common clinical condition. Increasing
with patient age, thyroid nodules are found in up to 20% of adults by
palpation and in up to 70% on sonographic studies; the malignancy
rate is 7-15% [1].
Non-palpable thyroid nodules may be found in about 50% of
patients with a clinically palpable solitary nodule, but they are also
incidentally detected by imaging studies performed for various
reasons [2].
Sonography is a choice of investigation in evaluation of thyroid
nodules. The high resolution of ultrasound has resulted in discovery
of large number of thyroid nodules which are obscure clinically.
Many ultrasound features have been described to differentiate benign
and malignant nature of the lesion [3].
Color and/or power Doppler ultrasound are useful to evaluate
vascularity of the thyroid gland and focal masses [4]. Although
sonographic guidelines have been established by society of
Radiologists in ultrasound, the American thyroid association and
European thyroid association, there is no specific ultrasound features in differentiating benign and malignant lesions [3].
Sonographic features that increase the likelihood that a nodule
is malignant include size, interval growth, marked hypoechogenicity,
and irregular margins and the presence of Microcalcifications,
lymphadenopathy, and local invasion of adjacent structures.
Prediction of malignancy using ultrasound remains difficult.
Since there is overlap of sonographic features between benign
and malignant thyroid nodules, ultrasound features are usually
corroborated with FNAC/Histopathology results in differentiating
various thyroid nodules [5].
Fine needle aspiration biopsy is considered the most reliable
diagnostic test for evaluation of thyroid nodules and has a low rate of
complications, especially when ultrasound guidance is used [4].
Recognition of specific morphologic patterns is an accurate
method of identifying benign thyroid nodules that may substantially
decrease the number of unnecessary biopsy procedures [5].
The goal in evaluating a thyroid nodule is to determine whether
it is benign or malignant so that patients with thyroid cancer can
receive a diagnosis and undergo treatment at an earlier stage to reduce
possible morbidity and mortality due to the disease, while avoiding
unnecessary tests and surgery in patients with benign nodules [6].
The purpose of this study is to evaluate accuracy of sonographic
morphologic feature oriented approach in identification of benign
and malignant thyroid nodule [3].
Current study designed to identify morphologic patterns on High
Resolution Sonography (HRS) those are predictive of benign and
malignant nodules and to evaluate the efficacy of histopathology and
HRS in differentiating benign and malignant nodules.
Materials and Methods
The study was conducted et at. R.L. Jalappa Hospital and Research
Centre, Tamaka, Kolar, Karnataka. We included all patients who were
diagnosed clinically with solitary thyroid nodule referred for USG of
the thyroid in R.L. Jalappa Hospital and Research Center during a
period of 18 months from December 2010 through May 2012.
High resolution ultrasonography of neck performed by using
SIEMENS G 40 & SIEMENS G 50 with 5-10 MHz transducers.
Thyroid sonographic findings relevant to benign or malignant
nodules were recorded.
The sonographic findings were compared with histopathology
reports of the thyroidectomy specimen.
Results
The present study deals with HRS of the thyroid that are
diagnosed clinically with solitary thyroid nodule and determination
of diagnostic accuracy of HRS with histopathology findings.
Benign lesions of STN were more common (70%) when compared
to malignant lesions (30%).
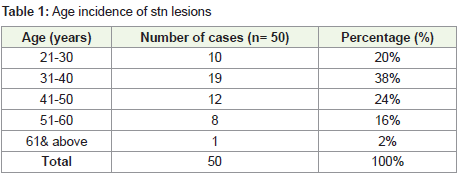
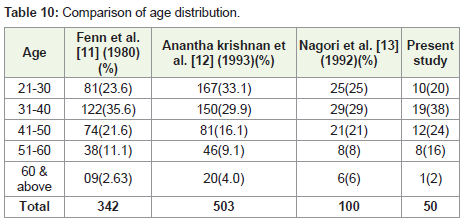
The commonest age group with thyroid pathology is between 31-
40 years (54%).
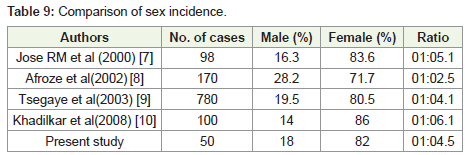
Out of 50 cases, 41(82 %) cases were females and 9(18%) cases
were males with male to female ratio of 1:4.5.
Nodules in the right lobe were more frequent and seen in 33(66%)
cases as compared to the left lobe seen in 15(30%) cases. Isthmus
lesions were seen in 2(4%) cases.
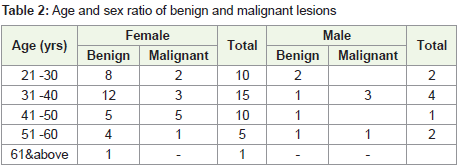
The female group showed occurrence of malignancy almost in all
from 3rd to 6th decade with maximum occurrence in 4th decade.
Out of 9 male patients 5 were benign nodules and 4 were
malignant nodules. In males malignant lesions were more common
in 3rd and 5th decade.
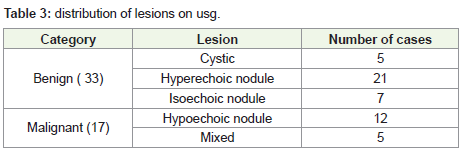
Out of 50 cases, histopathology revealed 35(70%) were benign
and 15(30%) were malignant.
The most common lesion was benign follicular adenoma 16
cases among benign lesions and papillary carcinoma 13 cases among
malignant lesions.
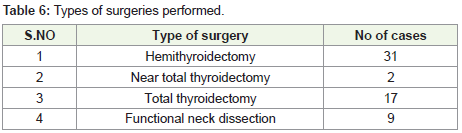
The commonest performed surgery in our series is
hemithyroidectomy, which accounts to 28(56%) cases. Functional
neck dissection was done in 3 cases of papillary carcinoma of thyroid
where lymph nodes were palpable.
Discussion
The number of males in the present study was 9 (18%) and the
females were 41 (82 %) with a male to female ratio of 1:4.5. Sex
distribution was similar when compared to Tsegaye et al. [9]. The
higher incidence of single nodules in females is more or less constant
for all age groups.
The incidence of STN is more common in females than males.
The highest age incidence in the present study as well as other
studies was between 21-50 years, the maximum being 31-40 years.
A solitary thyroid nodule presenting after 50 years of age
primarily neoplastic. The carcinoma in younger patients is more
often of a lower grade than in older patients who tend to have a more
aggressive form of malignancy.
Watters et al. (1992) 41 found that four specific morphologic
features are predictive of benign thyroid nodules were identified
which had 100% specificity for benignity.
• Spongiform configuration
• Cyst with colloid clot
• Giraffe pattern
• Diffuse hyperechogenicity
Watter et al. interpreted an USG report as suggestive of benign,
if the nodule was suggesting benign includes purely cystic/cystic with
thin septa, isoechogenicity, hyperechogenicity, well defined margins,
peripheral complete thin halo, comet tail artifact, egg shell/coarse
calcifications, peripheral vascularity
USG report as suggestive of malignancy includes Hypoechogenicity, Poorly defined margins, Taller than wide shape, Incomplete
peripheral halo, Microcalcifications, Intranodular vascularity
High resolution real-time USG is far better than clinical
examination in detecting thyroid nodularity.
Walker et al. have shown that the prevalence of multi nodularity
in clinically solitary thyroid nodules is between 20% and 40%, and
it has been observed that for a thyroid nodule to be detected by
palpation, it must be atleast 1 cm in diameter, while USG detects
nodules as small as 3 mm in diameter [16].
Conclusion
Solitary thyroid nodule is one of the commonest thyroid disorders.
Commonest presenting complaint is swelling in the anterior neck.
Solitary thyroid nodules commonly occur between 21-59 yrs age
group, the maximum being 31-40 yrs. Benign lesions are more
common than malignant lesions. Among benign, adenomas are the
most common lesions and among malignant, papillary carcinomas
are the most common lesions. Ultrasound features of thyroid nodules
are useful to distinguish patients with clinically significant thyroid
nodules from those with innocuous nodules despite the overlap of
findings. Sonographic findings can be useful when used alongside
cytological results, especially in nodules with cytological results that
are benign or suspicious for malignancy. Recognition of specific
morphologic patterns is an accurate method of identifying benign
thyroid nodules that may substantially decrease the number of
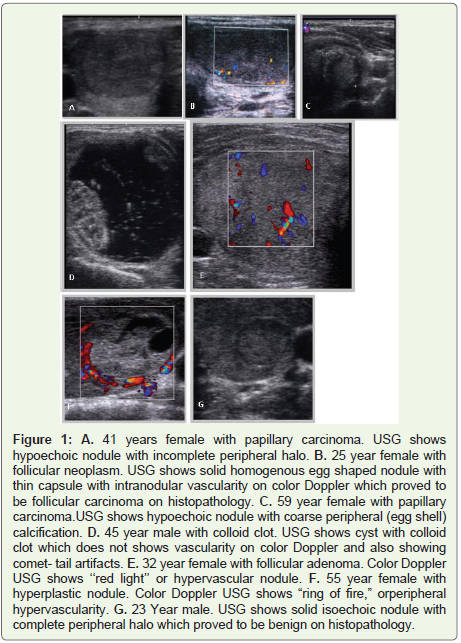
unnecessary biopsy procedures (Figure 1) and (Table 1-11).
References
Citation
Penaka H, Venkatesh M, Manjunatha YC. Role of High Resolution Ultrasonography Evaluation of Thyroid Nodules and Pathological 04 Correlation. Indian J Appl Radiol. 2019;5(1): 139.