Research Article
Role of Magnetic Resonance Spectroscopy in the Evaluation of Intracranial Brain Tumors on 3 Tesla MRI
Malpani P1, Pentyala S2 and Manchikanti V2*
1 Niloufer Hospital for Women and Children, India
2 Department of radiodiagnosis, Narayana medical college & hospital, India
*Corresponding author: Manchikanti V, Department of radiodiagnosis, Narayana medical college & hospital, Nellore-524 002, A.P, India
Copyright: © 2019 Malpani P, et al. This is an open access article distributed under the Creative Commons Attribution
License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is
properly cited.
Article Information: Submission: 09/07/2019; Accepted: 20/08/2019; Published: 22/08/2019
Abstract
Background: The present study is aimed to assess the contribution of MR spectroscopy in correlation with other MRI sequences towards the evaluation
of brain tumors and to diagnosing and grading the brain tumors with histopathological correlation.
Methodology: Analysis of spectra of 30 patients with brain tumors (27 intra axial and 3 extra axial) was done.
Results: 6 with GBM, 4 with anaplastic astrocytoma, 6 with diffuse infiltrative astrocytoma, 1 with oligodendroglioma, 1 with gliomatosis cerebri, 1 with
ependymoma, 5 with metastasis, 1 with choroid plexus papilloma, 1 with medulloblastoma,1 with lymphoma, 2 with vestibular schwannomas and 1 with
meningioma. Histopathology was not done in five cases. Five tumors didn’t correlate histopathologically. MRS of tumors shows decreased NAA levels since
neurons are superseded by the neoplasm cells. Furthermore, increase in choline levels are seen. Some tumors show Lac and Lip signals, which are markers
of anaerobic metabolism and necrosis. High Lac-Lip concentration helps to distinguish high and low grade gliomas. Glioblastomas have a higher Lac-Lip
concentration than anaplastic astrocytomas. Absence of the Lac-Lip signal does not exclude the diagnosis of high grade glioma. In our study peak Lac-Lip
was present in all the cases of glioblastoma in the necrotic component of the tumor. Cho contents measured with the Cho/Cr ratio increase with the grade of
astrocytoma. The decrease of Cho/Cr ratio in some glioblastoma is explained by the presence of necrosis in these tumours. No significant difference in NAA/
Cr ratio was observed in different types of gliomas. Other intraaxial brain tumors namely Gliomatosis cerebri, medulloblastoma, ependymoma and choroid
plexus papilloma showed elevated Cho/Cr and Cho/NAA ratios as well as decreased NAA/Cr ratios of varying degrees within the areas of hyperintensity on
T2-weighted images and in enhancing part of the tumor. In lymphoma, similar findings are found except for increased lipid-lactate peak. Extra-axial tumors
namely schwannoma and meningioma showed elevated Cho/Cr and Cho/NAA ratios as well as decreased NAA/Cr ratios of varying degrees and there was
an alanine peak detected in meningioma.
Conclusion: The study conclude that in vivo MR spectroscopy can be used as a reliable method for distinguishing neoplastic from non-neoplastic lesions
and also helpful in glioma grading. Some features of tumors on conventional MRI (e.g. contrast enhancement, surrounding edema, signal heterogeneity,
necrosis, haemorrhage and midline crossing) suggest a high grade. Accurate grading of gliomas on the basis of MRS alone may be difficult. Combining MRS
with conventional and other advanced MR imaging techniques, grading becomes more precise.
Keywords
Intraaxial brain tumors; MR spectroscopy; Glioma grading; Neoplastic lesions
Introduction
Intracranial tumors account for a significant proportion of
morbidity in our country and present several imaging challenges.
Primary brain cancers account for about 2% of all cancers. Apart
from these, brain and meninges are common sites of secondary
tumor implantation and their incidence increases with age.
Intracranial tumors account for a significant proportion of
morbidity in our country and present several imaging challenges.
Primary brain cancers account for about 2% of all cancers. Apart
from these, brain and meninges are common sites of secondary
tumor implantation and their incidence increases with age followed by Bangalore (2.8) [1].
Therefore, intracranial tumors form an important indication for
neuroimaging. Various modalities like plain radiograph, CT and MRI
are available for investigation of intracranial tumors. Imaging plays an
intrinsic role in intracranial tumor management. We are witnessing
a shift in imaging from merely providing anatomical information
towards providing information about tumor physiology [2].
Magnetic Resonance Imaging (MRI) has emerged as an important
diagnostic modality most frequently used to evaluate intracranial
tumors. Conventional MR imaging provides highly detailed anatomic
information helping in accurate depiction, delineation, treatment
planning and post treatment surveillance of intracerebral neoplasms.
In addition to conventional MR imaging techniques, a variety of
advanced techniques like MR spectroscopy, perfusion imaging,
Diffusion weighted Imaging (including DTI), Blood Oxygen Level
Dependent (BOLD) imaging and the emerging molecular imaging,
have found their place in clinical practice or are the subject of intense
research. These advanced techniques generate physiologic data and
information on tissue biochemistry.
Magnetic Resonance Spectroscopy (MRS) is an appealing noninvasive adjunct to MR imaging [3]. It’s a safe means of performing
biochemical analyses in vivo [4]. MR spectroscopy provides additional
information on the metabolic composition within an area of tissue. By
comparing the relative concentration of metabolites such as choline,
NAA, lactate etc., clinicians can judge factors like neuronal viability,
neurotoxins and membrane turnover within the volume of interest
and, thereby, the likely underlying pathology [3]. Widespread use of
faster MRS applications with higher Signal to Noise Ratio (SNR) and
spatial resolution allows us to detect functional metabolic changes,
thereby providing more information to understand the accurate
nature of the tumor and the morphological and physiological changes
occurring in the adjacent brain parenchyma.
This study is selected to assess the important role of MR
spectroscopy in the evaluation of brain tumors because when
diagnostic dilemmas present themselves, MRS considered in
perspective with MR imaging achieves a higher accuracy.
The multiplanar capability of MR imaging makes it the best
technique for evaluation of brain tumors and the anatomical
information from conventional MR sequences along with the
biochemical information from MR spectroscopy will help in better
assessment. This study was done in 30 patients on a 3T MR scanner.
Patients and Methods
Source of data: The main source of data for the study were
patients attending the department of Radiodiagnosis, Narayana
Medical College, Nellore.
Study design: Hospital based prospective study.
Sample size: The study is time bound study with sample size of 30 cases.
Method of collection of data:
All patients with clinically suspected brain tumors in a period of
2 years from Oct 2013 to October 2015 were subjected for the study.Nature of study:
The study involved adult patients and children and no normal
volunteers or pregnant women were included.Inclusion criteria:
• All patients with incidentally diagnosed brain tumors by CT.• Follow up patients of brain tumors.
• Clinically suspected cases.
• Cases of all age groups irrespective of sex.
Exclusion criteria:
• Patient having history of claustrophobia.• Patient having history of metallic implants insertion, cardiac
pacemakers and metallic foreign body in situ.
• Patient clinically unstable.
• Cases with benign lesions after histopathology confirmation.
Equipment: The conventional MRI and MRS scans were
performed on a 3 TESLA whole body scanner (GE medical systems
HDXT 750W) with a standard circularly polarised head coil during
the same examination session without repositioning the patient.
Sequences: Conventional axial T1W, T2W, SWI, DWI; coronal
FLAIR; Sagittal T1±post contrast T1 FSPGR axial, coronal and sagittal
sequences were taken. 2D PRESS 144 multi voxel spectroscopy was
performed at TE of 144ms and TR was at 1500 ms.
Cubic/nearly cubic MR spectroscopic voxels were centered over
solid portions of the lesions to sample the most metabolically active
tissue and to avoid necrotic debris with minimal contamination from
the surrounding non-tumoral tissue. The voxel was extended to cover
perilesional area in selective cases of high grade tumors.
The region of interest was defined by conventional T1 or T2W
sequences and post contrast sequence whenever done. Volume of
interest size ranged between 1.5x1.5x1.5 cm3
(3.4 ml) and 2x2x2 cm3
(8 ml). Spectroscopy was avoided in small lesions close to the bone
and sinuses.
Gadopentetate Dimeglumine contrast was used with dosage
being 0.1 mmol/kg bodyweight.
Study Definition
The resonance assignments were as follows:
Mobile lipids (Lip) at 0.9 - 1.4 ppm, Lactate doublet (Lac) at 1.15
- 1.50 ppm, Creatine (Cr) at 3.0 ppm, N-acetyl aspartate (NAA) at
2.02 ppm, Glutamate and glutamine (Glx) at 2.35 - 2.46 ppm, Choline
(Cho) at 3.2ppm, Myoinositol (mI) at 3.54 - 3.63 ppm and alanine at 1.4 ppm. An increase in choline peak, myoinositol peak, lipid
lactate peak and reduced NAA peak, creatinine peak was considered
significant for diagnosing brain tumors. In combination with
conventional MR sequences, we reported brain tumor as high grade
if there was increase in Cho/Cr ratio of more than 2.0, choline/NAA
ratio of more than 1.8, reduced NAA/Cr of less than 1.5. We reported
brain tumors as low grade if Cho/Cr ratio was less than
2.0, this value was used as a threshold value in order to increase
the specificity of detecting brain tumors.Statistical analysis:
Data was entered in Microsoft excel data sheet and analysis
was done. Descriptive statistics, frequencies and proportions were
calculated and tabulated. OPEN EPI software was used to calculate
sensitivity, specificity, negative predictive value, positive predictive
value and diagnostic accuracy to test the validity of MR Spectroscopy
with respect to histopathological examination. Fisher exact test was
the test of significance for categorical data. p<0.05 was considered as
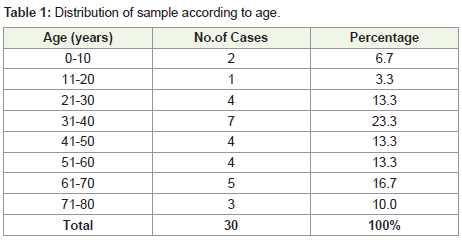
statistically significant (Table 1) (Figure 1and 2).In the study, majority of the patients i.e., 23% were between 31-40
years of age. The youngest patient was 2 year old with ependymoma
and the oldest was 79 year old with glioblastoma. In the study, the
majority i.e., 60% of the patients with intracranial brain tumors
were males. In the study, the majority of the tumors i.e 90% was in
intra-axial location. The majority of intra-axial tumors i.e 74% was in
supratentorial location. It was observed that majority of the tumors
i.e., 60% were well-defined and 40% were ill-defined with no definite
tumor margins.
In the study, it was observed that majority of the tumors i.e.,
showed perilesional edema. It is evident that most of the brain tumors
have perilesional edema.
In the study, it was observed that majority of the brain tumors
i.e., 63% were solid. 37% of the brain tumors were solid with cystic /
necrotic component within (Table 2).
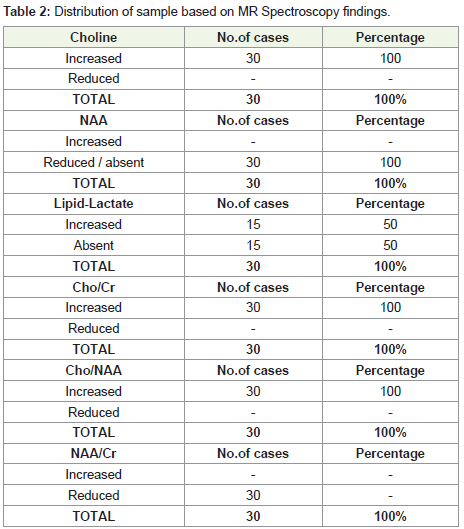
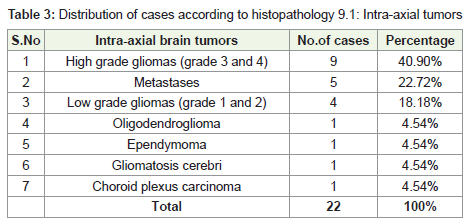
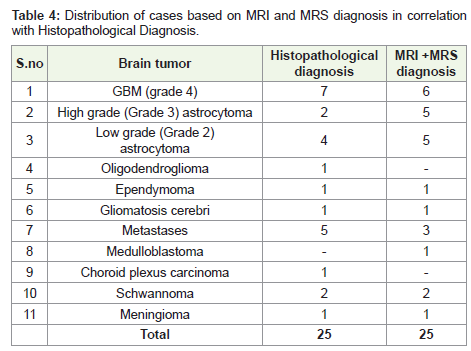
From the above findings, it can be inferred that all brain tumors
i.e 100% showed increased choline peak, Cho/Cr and Cho/NAA ratio
and absent or reduced NAA peak and reduced NAA/Cr ratio. In 50%
of cases, there was lipid lactate peak (Table 3 and 4).
There is significant association between MR spectroscopy
findings and histopathological findings for Glioblastoma Multiforme
(p<0.05).
There is significant association between MR spectroscopy findings
and histopathological findings for Anaplastic astrocytoma (p=0.03).
There is significant association between MR spectroscopy
findings and histopathological findings for Low grade astrocytoma
(p=0.0004).
There is significant association between MR spectroscopy findings
and histopathological findings for Ependymoma (p=0.04).
There is significant association between MR spectroscopy findings
and histopathological findings for Gliomatosis cerebri (p=0.04).
There is significant association between MR spectroscopy findings
and histopathological findings for Metastases (p=0.004).
There is no significant association between MR spectroscopy
findings and histopathological findings for Choroid plexus carcinoma.
There is significant association between MR spectroscopy findings
and histopathological findings for Schwannoma (p=0.0033).
There is significant association between MR spectroscopy findings
and histopathological findings for Meningioma (Table 5).
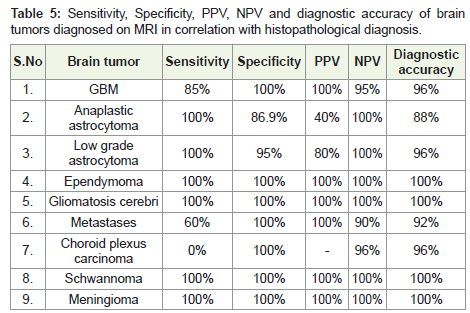
It can be inferred that for diagnosing intracranial brain tumors,
MRI with MR spectroscopy has 100% diagnostic accuracy in
diagnosing gliomatosis cerebri, ependymoma, meningioma and
schwannoma. Whereas diagnostic accuracy of 96% was observed
in low grade astrocytoma, GBM and choroid plexus carcinoma. A
diagnostic accuracy of 92% was observed in metastases and 88% in
anaplastic astrocytoma (Figure 3 and 4).
Discussion
Patients from all age groups were included in the study. Brain
tumors were most commonly found in the 31-40 (n=7) years age
group. The second most common age group was 61-70 (n=5) years
age group.
PA McKinney studied the incidence of brain neoplasms in all
age groups and found that primary brain neoplasms occur most
commonly in 7th decade [5]. Out of the 30 patients present in the
study, the incidence of intracranial brain neoplasms was more in
males 60% (n=18) compared to females.
Krishnatreya et al. attempted to identify the epidemiology of
primary malignant brain tumors in North-east India with data from
a hospital cancer registry and their analysis showed a male-female
ratio of 2.3:1 [6].
In the study of 30 cases, intra-axial tumors were more commonly
present (n=27) and evaluated with MR spectroscopy than the extraaxial tumors (n=3). Out of the 27 intra-axial tumors, 74% (n=20)
were supratentorial, 15% (n=4) were infratentorial and 11% (n=3)
were combined supra and infratentorial. Intra-axial supratentorial
tumors were more common in the study.
Out of the 30 cases present in the study, majority of the brain
neoplasms were solid 63% (n=19) and the remaining were solid with
cystic/necrotic component within 37% (n=11).
Gliomas were the most common brain neoplasm found in the
study and constituted 63.33% (n=19) of the total 30 cases. Out of 19
cases of gliomas diagnosed on MRI, 6 were GBM, 4 were anaplastic
astrocytoma, 6 were diffuse infiltrative astrocytoma, 1 case was
of oligodendroglioma, 1 case of gliomatosis cerebri and 1 case of
ependymoma.In the study, 17 out of 19 (95%) cases of glioma had
perilesional edema. The cases which did not show perilesional edema
were ependymoma (n=1) and a low grade glioma (n=1).
Dua RK et al. studied the expression of aquaporin-4 in 30 cases of
brain tumors and concluded aquaporin-4 expression was increased
in brain tumors compared to normal brain and that it could be
playing a role in alteration of blood- brain barrier leading to contrast
enhancement and perilesional edema [7].
In the study, most of the GBM and anaplastic astrocytoma cases
were heterogenous lesions with both solid and necrotic components.
4 cases of diffuse infiltrative astrocytoma and 1 case of ependymoma
were solid lesions showing no necrotic center.1 case of low grade
glioma was a cystic lesion with solid mural nodule. The case of
gliomatosis cerebri was solid.
In the study, all GBM showed moderate to intense heterogenous
enhancement, anaplastic astrocytomas showed no obvious to
mild enhancement, and diffuse infiltrative astrocytoma cases had
minimal enhancement. Ependymoma showed homogenous intense
enhancement and a case of gliomatosis cerebri showed no obvious
enhancement.
The findings are in agreement with study conducted by R Felix,
W Schörner et al. Histopathology was done in 18 out of 19 cases
of gliomas [8]. MRI findings correlated with histopathology in 14
out of 18 cases. First case which did not correlate was of anaplastic
astrocytoma which turned out to be anaplastic oligodendroglioma
on histopathology. Second case was of a butterfly glioma given
as anaplastic astrocytoma based on MRI and MRS findings but
turned out to be grade 4 glioma on histopathology. Third case was
of a low grade glioma, which turned out to be metastatic papillary adenocarcinoma deposit on histopathology. The fourth case was of
a high grade glioma, which on histopathology turned out to be a
follicular thyroid carcinoma deposit. Histopathology was not done in
a case of hypothalamic glioma (n=1).
The cut-off value of Cho/Cr ratio>2.0 helped in accurate grading
of the gliomas into high and low grades in 17 cases except for 1 case
of high grade glioma which showed Cho/Cr <2.0 and 1 case of low
grade with ratio >2.0.
Low Grade Astrocytoma (LGA) is less common than anaplastic
astrocytoma and GBM, accounting for between 10-15% of
astrocytomas in adults. Diffuse infiltrative astrocytoma are grade 2
astrocytomas.
There were 6 patients with diffuse astrocytoma in the study within
the age group of 19 years to 53 years. Seizures was the most common
presentation of the patients.
Most of the lesions were hypointense on T1W and hyperintense
on T2W MR sequences. Lesions were solid to solid and cystic. Most of
the lesions were well- defined. 5 lesions were supratentorial and one
was infratentorial. On contrast study, the lesions showed minimal to
mild enhancement. Post contrast study was not done in one of the
patients. No blooming was observed on SWI sequence.
On MRS, the six tumors showed increased choline peak, reduced
NAA and increased mI peak. There was increased Cho/Cr ratio in all
the cases with ratio >2.0 in one of the cases and being <2.0 in five cases.
The Cho/NAA ratio was increased in all the cases compared to the
normal brain parenchyma being 2.2(±0.6) and there was decreased
NAA/Cr ratio in all the cases. mI/Cr ratio was higher at 0.9(±0.3).
Histopathology didn’t correlate in one of the case, it was biased
towards low grade glioma based only on MRI findings of lack of
perilesional edema and mild enhancement and MRS findings (elevated
lipid lactate and raised Cho/Cr of 2.6) were ignored. But it turned out
to be papillary adenocarcinoma metastatic deposit. Consideration
of MRS findings might had helped in arriving to a more appropriate
diagnosis. Histopathology was not done in one case
However, the diagnostic accuracy was 96% and there was a
significant association between MRS and histopathology findings
with p=0.0004 (p<0.05 being significant). The sensitivity was 100%
and specificity was 95%.
Meng Law et al. in their study on gliomas, gave the metabolite
ratios range for low grade gliomas as Cho/Cr 0.85-4.0, Cho/NAA 0.6-
6.8 and NAA/Cr 0.33-3.6 [9].
Mauricio Castilloa et al, in their study on mI levels in cerebral
astrocytomas, showed a trend towards lower mI levels in the presence
of anaplastic astrocytomas (mI/Cr 0.33±0.16) and GBMs (mI/Cr
0.15±0.12) compared with those of low-grade astrocytomas (mI/Cr
0.82±0.25) [10].
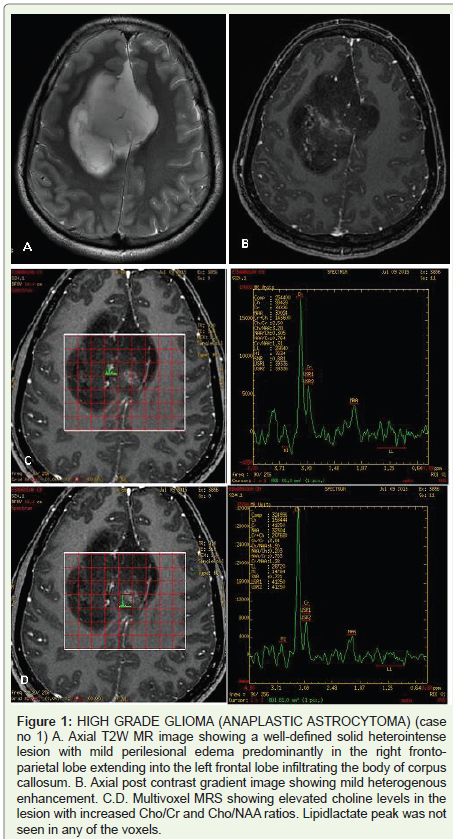
Anaplastic astrocytomas represent one-third of all astrocytomas,
second in frequency only to GBM. Anaplastic astrocytomas are WHO
grade III tumors, intermediate in malignancy between LGA (WHO
grade II) and GBM (WHO grade IV). Five patients with anaplastic
astrocytoma were evaluated in the study. Three were in 4th decade and
one each in the 3rd and 6th decades of life.
The lesions were all supratentorial and hypo to isointense on
T1W and iso to heterointense on T2W conventional MR sequences.
SWI blooming was seen in one of the lesions. The lesions showed no
obvious to mild enhancement. Contrast study was not done in two of
the patients
There was a case of butterfly glioma, in the 3rd decade, in which
the lesion was seen crossing the midline via the corpus callosum
anteriorly. Diffusion tensor imaging was done which showed the
disruption of white matter tracts in the corpus callosum.
On MRS, the tumors showed significant increase in choline,
correlating well with the high cell density in these tumors. The tumors
also showed reduced NAA and reduced Cr peak. There was reduced
mI peak in one and increased mI peak in the other three. There was
increased Cho/Cr ratio of >2.0 in four of the cases and <2.0 in one
of the cases. There was increased Cho/NAA and decreased NAA/Cr
ratios in all the five cases. Two of the cases showed increased choline
peak with raised Cho/Cr ratio in perilesional edema probably due to
tumoral infiltration.
Histopathology findings correlated in two of the five cases and
did not correlate in the other three. One turned out to be anaplastic
oligodendroglioma. The butterfly glioma turned out to be grade 4
glioma which was diagnosed as anaplastic astrocytoma based on the
MRS findings as there was no lipid lactate peak indicating necrosis
in any of the tumor voxels placed in the enhancing or the nonenhancing part. The other case which turned out to be a follicular
carcinoma thyroid metastatic deposit was diagnosed as high grade
glioma based on MRI and MRS findings as the lesion was solitary
with extensive perilesional edema and high Cho/Cr and Cho/NAA
ratios with elevated lipidlactate peak.
The diagnostic accuracy turned out to be 88% with sensitivity
of 100% and specificity of 87% but a low positive predictive value
of 40%. There was significant association between MR spectroscopy
findings and histopathological findings, with p=0.03.
Glioblastoma multiforme is the most common primary brain
tumor and the most malignant of the astrocytomas. GBM are WHO
grade IV neoplasms.
6 patients with GBM were evaluated in the study. All the cases
were adults with most being in the 6th to 8th decades. Seizures and focal
neurological deficits were the most common presenting symptoms.
All the cases were supra-tentorial and appeared hypo to heterointense on T1W and hetero-intense on T2W conventional MR
sequences. Most of the cases were combined solid and cystic. They
were predominantly ill-defined with moderate to extensive vasogenic
edema. Blooming was a prominent feature observed in 5 of the 6
cases. All the cases showed enhancement on post contrast gradient
sequence but the enhancement was irregular and heterogenous.
There were one case of butterfly glioma in 8th decade, in which
the lesion was seen crossing the midline via the corpus callosum
posteriorly.
Gliomatosis cerebri is a distinct entity of glial tumors characterized
by diffuse infiltration of the glial cell neoplasm throughout the brain.
The WHO classification denotes grades II, III and IV gliomatosis
cerebri [11].
The study includes one patient with gliomatosis cerebri, in the
4th decade, who presented after experiencing the first instance of a
generalised seizure. On conventional MR sequences, the lesion was
diffusely infiltrating subtle T1 hypointense and T2 hyperintense in
both frontal and parietal lobes. The lesion was ill-defined and showed
no enhancement on post contrast gradient echo T1 sequence. No
blooming was seen on SWI sequence.
On MRS, the tumor showed increased choline peak, reduced
NAA, increased mI peak and mildly elevated Cr peak. There was
increased Cho/Cr ratio of 2.0, increased Cho/NAA ratio of 2.4 and
reduced NAA/Cr ratio of 0.9. mI/Cr ratio was higher at 0.80.
Martin Bendszus et al. evaluated 8 patients with gliomatosis
cerebri and found elevated Cho/Cr and Cho/NAA as well as
varying degrees of decreased NAA/Cr ratios [12], which were most
pronounced in the anaplastic lesions.
Damien Galanaud et al. studied 9 patients affected with
gliomatosis cerebri and confirmed markedly elevated levels of Cr
and mI [13], reduced levels of NAA and a moderately elevated level
of Cho. And also studies done by Mohana-Borges et al. and PerettiViton P et al. [14,15].
In our study, intermediate TE was used, so mI level was not
appreciately accurately as it is a short TE metabolite.
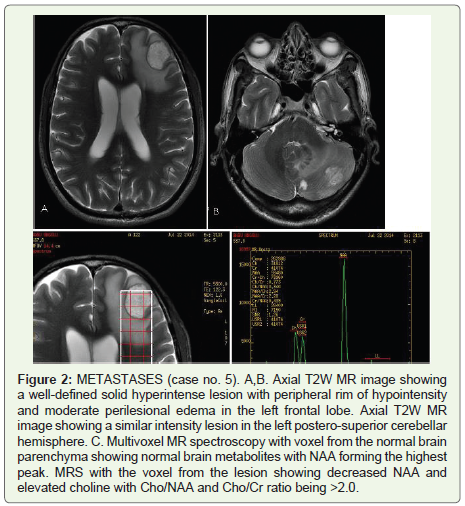
Brain metastases are not only a leading cause of cancer mortality
but as a group have become the most common CNS neoplasm
in adults. The brain parenchyma is the most common site (80%),
followed by the skull and dura (15%). Although they usually do not
pose much of a diagnostic challenge when they are multiple, based
on conventional MRI, metastases can be problematic when they are
solitary because it may be difficult to distinguish them from primary
brain neoplasms [16].
5 cases of metastases were evaluated in the study. They were in
5th, 6th and 7th decades. Headache, seizures and focal neurological
deficits were the most common presenting symptoms. Histopathology
was not done in two cases.
On MRS, strong Cho peak was seen without elevation in
surrounding peritumoral edema. The lesions showed reduced NAA
and Cr. Increased lipid/lac peak in two of the tumors. There was
increased Cho/Cr ratio of >2.0 in 4 cases and <2.0 in 1 case with
the mean Cho/Cr ratio being 2.0(±0.55), increased Cho/NAA ratio
in all cases with ratio being 2.1(±0.3) and reduced NAA/Cr ratio at
0.9(±0.4).
Cho/Cr ratio was not elevated in peritumoral edema.
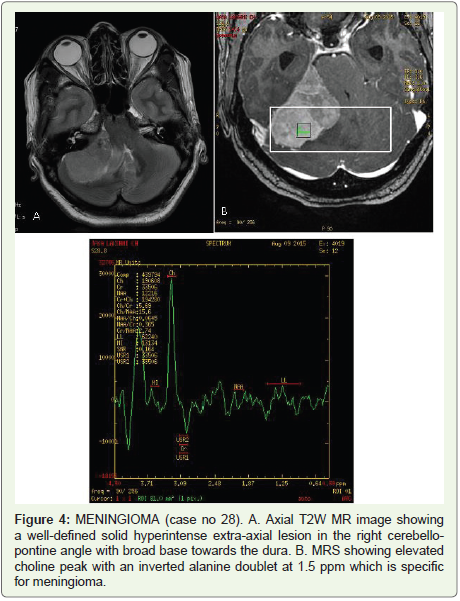
Meningioma is the most common intracranial extra-axial tumour
in adults, but is the second most frequent lesion in the CerebelloPontine (CP) angle after vestibular schwannoma, representing 10%-
15% of all tumours in this location[17].
Proton MR Spectroscopy, at intermediate TE=144 ms, showed
a marked reduction in NAA and Cr, elevated choline peak with the
characteristic presence of a negative doublet of alanine observed at
1.5 ppm. There was elevated Cho/Cr, Cho/NAA and reduced NAA/
Cr ratio.
There was a diagnostic accuracy of 100% and significant
association between MR Spectroscopy findings and histopathological
findings for meningioma with p=0.04 (p<0.05 being significant).
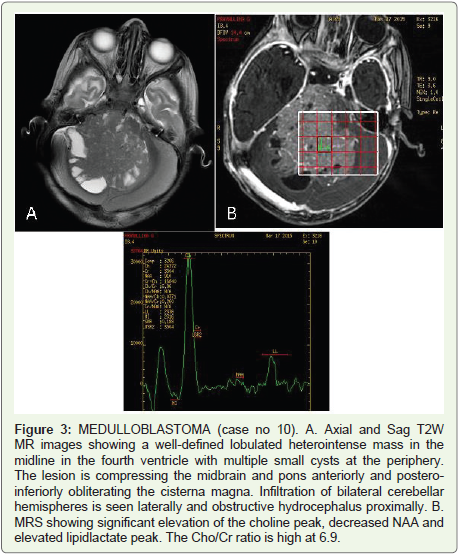
Medulloblastoma (MB), a highly malignant neoplasm, is the most
common posterior fossa neoplasm in children, representing 15% to
20% of all pediatric brain tumors and 30% to 40% of posterior fossa
neoplasms [18,19].
Based on MRI and MRS findings, a diagnosis of medulloblastoma
was made. But the histopathological and immunohistochemical
findings diagnosed it as choroid plexus carcinoma.
The specificity was 100% but the sensitivity was 0% and there
was no significant association between MRI and histopathological
findings (p=1.000).
Lymphoma of the CNS consists of 2 major subtypes: secondary
CNS involvement by systemic lymphoma (the most common) and
primary CNS lymphoma, in which the lymphoma is restricted to
the brain, leptomeninges, spinal cord, or eyes, without evidence of it
outside the CNS at primary diagnosis [20].
The study included an 8th decade female presenting with altered
mental status and neuropsychiatric disturbances.
On MRS, increase in choline, reduction in NAA and creatine was
seen. There was also increased Cho/Cr ratio of 1.6, increased Cho/
NAA ratio of 1.8 and decreased NAA/Cr ratio of 0.8. Lipid lactate
peak was not elevated.
However, based on conventional MRI findings, a diagnosis of
lymphoma was made. The study done is partly in agreement with
previous study done by:
MRS in a case series by Asem Mansour et al. on 21 patients with
lymphoma, consistently showed increased choline and decreased
NAA along with the presence of lipid peak[21].
Conclusion
The study conclude that in vivo MR spectroscopy can be used as
a reliable method for distinguishing neoplastic from non-neoplastic
lesions and also helpful in glioma grading. Some features of tumors on
conventional MRI (e.g. contrast enhancement, surrounding edema,
signal heterogeneity, necrosis, haemorrhage and midline crossing)
suggest a high grade. Accurate grading of gliomas on the basis of MRS
alone may be difficult. Combining MRS with conventional and other
advanced MR imaging techniques, grading becomes more precise.
The study also demonstrates that spectroscopic MR measurements
in the peritumoral region can be used to demonstrate peritumoral
infiltrative nature of certain intraaxial brain tumors.
References
1. Yeole BB (2008) Trends in the brain cancer incidence in India. Asian Pac J
Cancer Prev 9: 267-270.
Citation
Malpani P, Pentyala S, Manchikanti V. Role of Magnetic Resonance Spectroscopy in the Evaluation of Intracranial Brain Tumors on 3 Tesla
03 MRI. Indian J Appl Radiol. 2019;5(1): 136.