Case Report
Aberrant Vertebral Artery Causing High Cervical Myelopathy: Case Report
Nikam V1, Nagure P2* and Patil J3
1Department of Anatomy, D.Y. Patil Medical College, India
2Department of Radiodiagnosis, Prakash Institute of Medical Sciences, Consultant Radiologist at Eureka Diagnostic Centre, India
3Department of Radiodiagnosis; D. Y. Patil Medical College, India
*Corresponding author: Nagure P, Consultant at Eureka Diagnostic Centre, Department of Radiodiagnosis, Prakash Institute of Medical Sciences, Urun Islampur, India, Mobile no: +91-7387034090; E-mail: drnagurepramod@gmail.com
Copyright: © 2019 Nikam V, et al. This is an open access article distributed under the Creative Commons Attribution
License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is
properly cited.
Article Information: Submission: 07/05/2019; Accepted: 27/06/2019; Published: 01/07/2019
Abstract
The vertebral arteries are commonly affected by anatomical variations. Here we report an anomalous and aberrant intradural course of left vertebral
artery leading to compression of upper part of spinal cord at cervico-medullary junction and involving the spinal nucleus of trigeminal nerve. This leads to the
involvement of motor tracts and trigeminal nerve.
Keywords
Trigeminal hypesthesia; Cervical myelopathy; Vertebral artery anomaly; Anatomical variation
Introduction
The vertebral artery arises on both the sides from the first part of
the subclavian artery at the root of the neck and proceeds superior and
posteriorly in the interval between the vertical part of the longus colli
and anterior scalene muscles to the level of the 6th cervical vertebra.
The artery passes upwards through the transverse foramen of the
6th cervical vertebra and all succeeding transverse foramina. After
leaving the transverse foramen of the atlas, the vertebral artery turns
posteromedial and passes in a groove along the posterior arch of atlas.
Then the vertebral artery turns anteriorly to enter the vertebral canal,
penetrates the dura mater, enters through the foramen magnum, and
runs superiorly along the anterior surface of the medulla oblongata to
the inferior aspect of the pons. Here it joins the vertebral artery from
the opposite side in the midline to form the basilar artery.
With opposite artery it supplies deep neck muscles, spinal cord
and posterior part of the brain supplying the brainstem, cerebellum, thalamus, occipital lobe and temporal lobe of the cerebral cortex [1,2].
The vertebral arteries are widely known to be variable in their
course. This can lead to difficulty in the surgical management of many
conditions of the cervical spine disorders. Occasionally abnormalities
of the vertebral arteries themselves indicate and become symptomatic.
Vertebral artery abnormalities have been reported to cause many of
symptoms such as neck and arm pain [3,4].
Anomalous origin of vertebral artery is not very usual finding
with the prevalence ranging from 3-8% [5,6]. Though vertebral artery
anomaly is unusual, a report from a series of 300 vertebral artery
anomalies and most of the cases are asymptomatic but few cases have
been reported with cervical pain, occipital pain and myelopathy [7].
Here we report a rare case of high-level cervical cord compressive
myelopathy and ipsilateral facial hypaesthesia due to anomalous left
vertebral artery.
Case Report
A 40 years old male non-hypertensive, non-diabetic presented
with progressive weakness in all four limbs and progressive complaints
of headache, dizziness, left facial progressive weakness since 15 days.
No history of vertigo, fever, recent travel or loose motions.
On examination patient was alert, conscious but presented with
quadriparesis. The cranial nerves were intact but decreased sensation
to touch and temperature in left C1, C2 and C3 segments distribution.
The deep tendon reflexes were exerted with mild spasticity.
Speech and memory was intact. The patient was advised for MRI
brain; MRI angiography with cranio-vertebral junction.
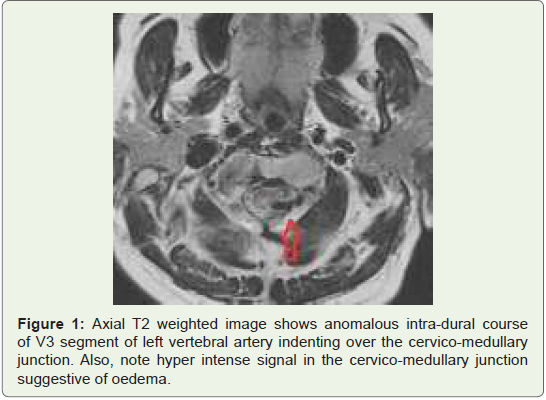
MRI Brain showed the intradural course of V3 segment of left
vertebral artery, which was indenting over the cervico medullary
junction. The left vertebral artery was passing posteromedially and
intradurally between the axis and atlas and above the C1 vertebra’s
foramen transversarium and impinging on the upper segments of
spinal cord. The image also showed a hyper intense signal in the cervicomedullary
junction, which was suggestive of oedema (Figure 1).
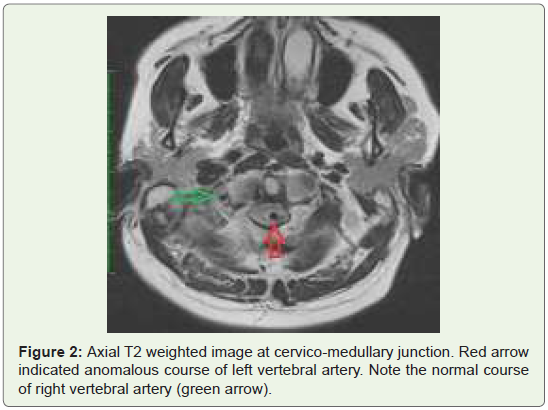
The course of right vertebral artery was normal Figure 2.
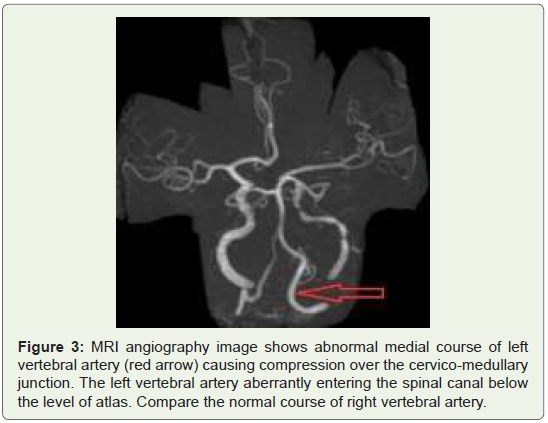
The MRI angiography image demonstrated the anomalous course
of left vertebral artery with cervico-medullary compression Figure 1and ).
After MRI brain and MRI angiography, the patient was referred
to Neurophysician for further management.
Discussion
Knowing the anatomical abnormalities, no matter how rare but
still necessary for perfect diagnosis and treatment of patients. The
vertebral artery is linked with several anatomical variations for e.g. -
in approximately 4-6% of subjects the left vertebral artery arises from
the aortic arch [1,8]. Further, in 60-70% of the subject the vertebral
artery is of different size, with left more frequently larger than the
right [2,3]. Seldom is a single vertebral artery present, or one fails to
reach the opposite vessel to form the basilar artery [8]. Even though
abnormalities of the vertebral artery may not be common, reports of
deficits due to the extra cranial neural compression are seen. Most of
the patients come with symptoms of irritation or injury to the nerve
root or cranial nerve deficits [4]. MRI, CT angiography or cerebral
angiography are the choice of investigations to diagnose such patients [7]. In our case, also we investigated the patient by MRI.
In our case there was cord compression at cervico-medullary
junction with involvement of spinal nucleus of trigeminal nerve;
as the patient complained of progressive weakness of all four
limbs indicating the lesion of pyramidal tracts as well as there was
left hypesthesia of the face and forehead with loss of touch and
temperature.
Imaging of the cervical spine showed the abnormal course of
left vertebral artery dorsal to spinal cord. Continuous pulsations of
the artery for a longer duration might be the cause of compressive
myopathy in our case, there might be sporadic and irregular
stimulation of the spinal cord by the abnormal course of left vertebral
artery involving the spinal nucleus of trigeminal nerve which lies in
the higher segments of spinal cord and this correlates with the loss of
exteroceptive sensations on the ipsilateral side of face and forehead.
Structural anomalies of the vertebrobasilar system can create a
variety of neurological symptoms. In such cases of direct compression, neural structures by the vertebra-basilar system and pulsatile character
of arterial blood flow can produce cranial nerve or ponto-medullary
dysfunction, cervical myopathy or cervical radiculopathy [9].
Classically Jannetta related vascular compression of the trigeminal
nerve to trigeminal neuralgia and conveyed that microvascular
decompression of the affected nerve could induce symptomatic relief
[10]. In these cases, trigeminal nerve dysfunction is secondary to
compression of the caudal part of spinal nucleus of trigeminal nerve.
In present study also, there was the compression of upper part of
spinal cord segments involving the spino-medullary junction.
Cervical myelopathy may be precipitated by vertebral artery
tortuosity; such abnormalities may be more frequently symptomatic
which though generous is not ideal, as the spinal canal at the
foramen magnum cannot provide a space to an intruding vascular
structure without cervical cord compression [11]. In present study
also, tortuosity of abnormal course of left vertebral artery may be the
prime reason for the myelopathy and cord compression leading to
involvement of spinal nucleus of trigeminal nerve and motor fibres,
which lead to weakness in limbs and face.
The bilateral VA normally develop from the distal part of the 7th
dorsal intersegmental arteries. Anatomical variations of VA arise from
persistence or obliteration of these arch arteries and intersegmental
arteries. Anomalous origin of VA occurs when there is aberrant
anastomosis during the embryonic development of the arch. The site
of anastomosis will define the eventual unusual origin. However, the
difference in the entry level of VA is related to the dominance of a
ventral or dorsal intersegmental anastomosis.
Intradural course of C1-C2 VA means the VA courses
posteromedially after the exiting the C2 transverse foramen and
pierce the spinal canal between C1 and C2 not traversing through
C1 transverse foramen, this was present in our case also. The
embryological explanation is the first intersegmental artery remains
without persistence of the first VA.
Congenital osseous anomalies such as hypoplastic odontoid,
Os odontoideum and bifid C1 posterior arch have been reported to
increase the incidence of intradural course C1-C2 VA [11-14].
However, in our case no osseous anomalies and variation in the
origin of left vertebral artery was present but there was anomalous
course of left vertebral artery at C1-C2; which represents the first
intersegmental artery.
Conclusion
Anomalies of vertebral artery can cause disturbances in vertebrabasilar
blood supply and related to anatomic position of anomalous
vertebral artery, cervical and spino-medullary junction may produce vascular complications. Thus, abnormal course of vertebral artery
should be a part of differential diagnosis of upper cervical lesions
presenting the symptoms of myelopathy in limbs and on face.
Microvascular decompression around the vertebral artery could
be sufficient and safe method to indirectly decompress the spinal
cord.
References
Citation
Nikam V, Nagure P, Patil J. Aberrant Vertebral Artery Causing High Cervical Myelopathy: Case Report. Indian J Appl Radiol. 2019;5(1): 134.