Case Report
Acardiac Fetus: Twin Reversed Arterial Perfusion Sequence, A Rare Entity!
Kumra M*, Lakhkar DL and Kachewar SG
Department of Radiodiagnosis, DVVPF’S Medical College and Hospital Ahmednagar, India
Corresponding author: Kumra M, Junior Resident, Department of Radiodiagnosis, DVVPF’S Medical College and Hospital Ahmednagar, Maharashtra, India, Tel no: +91-9910314624; E-mail: drmeghakumra@gmail.com
Citation: Kumra M, Lakhkar DL, Kachewar SG. Acardiac Fetus: Twin Reversed Arterial Perfusion Sequence, A Rare Entity!. Indian J Appl Radiol. 2018;4(1): 130.
Copyright ©2018 Kumra M, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Indian Journal of Applied Radiology | Volume: 4, Issue: 1
Submission: 01/10/2018; Accepted: 19/11/2018; Published: 23/11/2018
Abstract
Heart is the organ which is essential to life. Twin Reversed Arterial Perfusion Sequence (TRAP) is a rare complication of monochorionic twin pregnancy, in which one twin develops without formation of a heart or heart like structure and it survives till it does as it is supported by the second twin which acts as donor via anomalous anastomosis. The reported incidence is 1 in 35,000 births and 1 in 100 in monozygotic monochorionic twin pregnancies. The diagnosis is made antenatally with characteristic grey scale and Doppler sonography findings. Due to high mortality risk, diagnosing TRAP is essential to plan early intervention and better outcome of the donor twin. Pertaining to its rarity, we report a case of 27 weeks twin gestational pregnancy with presence of an acardiac TRAP sequence twin. The clinical presentation, imaging findings, outcome, prognosis and treatment are reviewed in the article under the light of literature, to emphasize the importance of ultrasonography as a simple but adequate tool not only in the diagnosis and follow-up but also in management of such a case.
Introduction
Congenital anomalies are known to be relatively more common in multi-fetal pregnancies. One of the rare anomalies found in monochorionic twin pregnancy is the Twin Reversed Arterial Perfusion Sequence (TRAP), the hallmark of which is one twin which develops without a heart, known as the “acardiac twin” and the second twin, known as the “pump twin” which acts as a donor by perfusing the acardiac twin via arterial to arterial anomalous anastomosis in the reversed direction [1]. The reported incidence is 1 in 35,000 births and 1 in 100 in monozygotic monochorionic twin pregnancies [2]. The pump twin is usually normal, the other is an abnormal mass of tissue, consisting usually of legs and a lower body, but no upper body, head or heart, as in our case, having no chance of survival and causing a poor prognosis of the donor twin. The diagnosis is made antenatally with characteristic grey scale and Doppler sonography. Identification of dysmorphic features of along with reversed flow in umblical arteries of the affected fetus help in the diagnosis. Early diagnosis of TRAP is essential so that intervention can be planned early in the pregnancy for a better outcome of the pump twin [3].
Case Report
A 20 year old female primigravida patient having 27 weeks of amenorrhea with a pre-diagnosis of twin gestation with fetal anomaly from a peripheral center was referred to our Department of Radiology for advanced ultrasonography and Doppler examination. Her medical history and family history were non-significant and she was not suffering from any systemic diseases.
Imaging findings
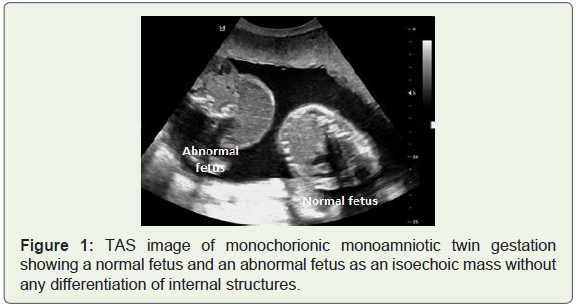
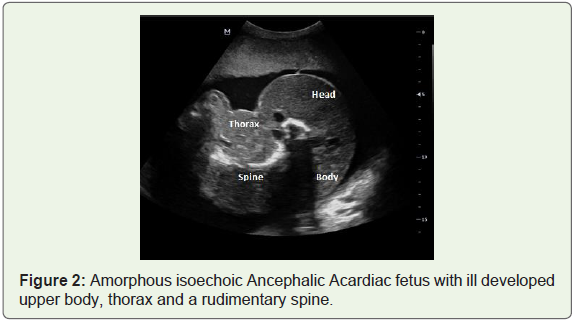
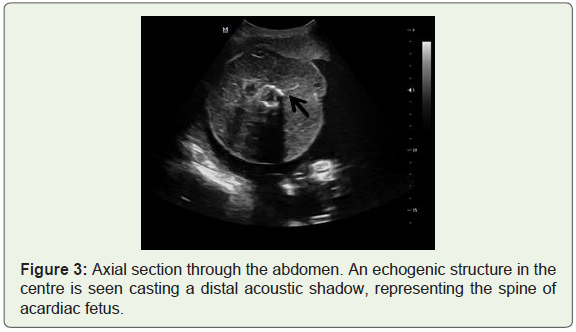
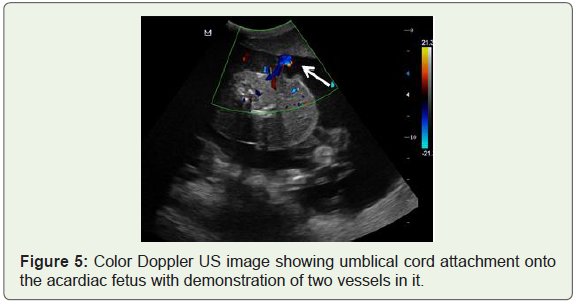
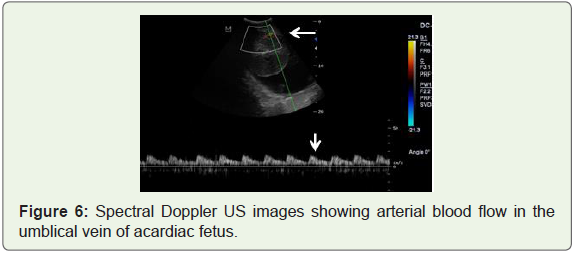
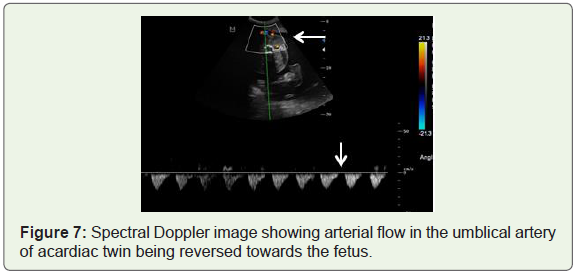
On ultrasonography, an intrauterine monochorionic monoamniotic twin pregnancy was observed (Figure 1). One twin appeared normal visually while the other twin appeared malformed. The amniotic fluid was on a higher side than normal for the age. A single placenta was seen on the anterior wall of upper segment of uterine cavity. Cardiac activity was noted in the first fetus and biometric measurements were taken and gestational age of normal fetus wasaveraged to 26 weeks and 4 days. No anomalies were detected in first fetus. Umblical cord of this fetus showed three vessels with normal color Doppler and waveforms on spectral Doppler. The second fetus was an abnormal/amorphous mass of tissue, consisting of an underdeveloped thorax, a relatively well definedlower body and lower limbs (Figure 2). Lower limbs were seen flexed and folded over one another with clubbed feet. There was no head, heart or heart like structure seen. Cardiac activity was not appreciated in the rudimentary thorax of the second fetus. Fetal cranium was not appreciated; hence Biparietal diameter and Head Circumference could not be measured. The fetal abdomen was surrounded with a large hydrops ring and the lengths of the extremities were consistent with 23 weeks and 2 days (Figure 3,Figure 4). Umbilical circulation of second fetus was well seen around the abdomen. There was presence of two vesseled umblical cord (Figure 5). On spectral Doppler USG, the umblical vessels showed arterial waveforms in both umbilical artery and vein and the direction of flow of blood in the umblical artery wasreversed i.e. towards the fetus as demonstrated by the negative waveform on spectral Doppler (Figure 6,Figure 7). Under the light of these observations, twin to twin transfusion syndrome and TRAP sequence were considered.

Outcome
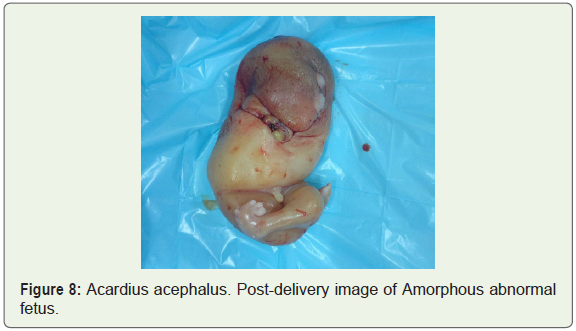
The patient was monitored with weekly ultrasonographic and Doppler examinations to assess the wellbeing of normal twin. At about 28 weeks of gestational age, patient experienced PV leaking and was kept under-observation. She eventually went into spontaneous pre-term labor 2 days later and vaginal delivery was planned. The first normal twin attained cephalic lie and vertex presentation at that time and was delivered uneventfully. It was a live male baby weighing about 1000 gms. He cried immediately after birth with APGAR scores of 1 and 4 in the first and fifth minutes and immediately shifted to the neonatal intensive care unit. The second twin was subsequently delivered vaginally with the help of obstetric maneuvers followed by delivery of the placenta (Figure 8). The normal pump twin could not survive and died 2 days later despite intensive care.
Pathologic findings
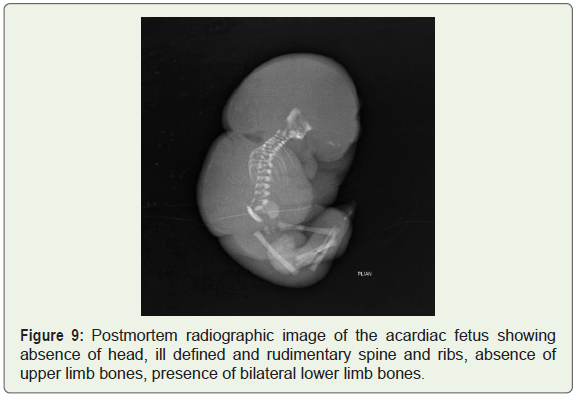
The Postmortem radiography of the acardiac twin along with contrast study of placental circulation was done. The radiography showed acrania, absence of upper limbs and ill-defined spine and ribs. In the lower limbs, femur, tibia and fibula were seen bilaterally (Figure 9).
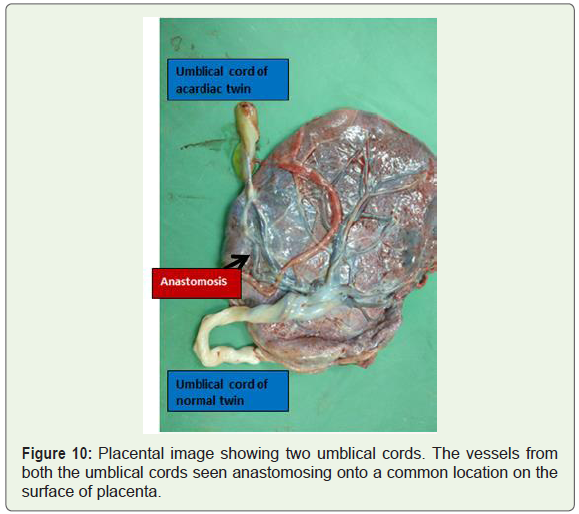
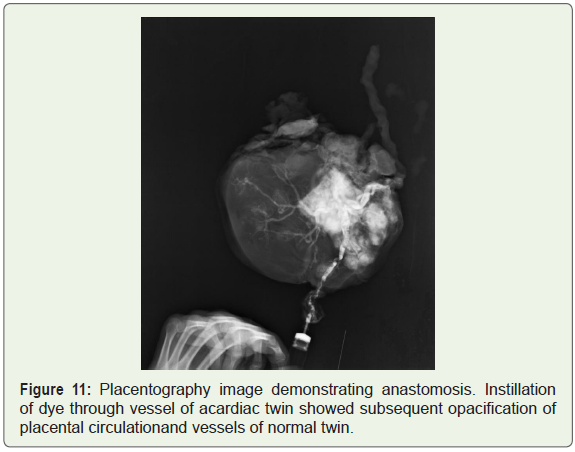
Placenta was visually assessed and on the fetal surface of placenta, a vessel supplying the acardiac twin was seen anastomosing with the root of umblical vessels of normal twin (Figure 10). On placentography, dye was pushed from the umblical artery of acardiac fetus and it was seen to fill the entire placenta and opacifying the circulation of vessels of normal twin as well thus confirming the presence of anastomosis (Figure 11).
Discussion
Acardiac twinis a very rare congenital anomaly occurring in monochorionic twin pregnancy. It was first described by Benedetti in 1533. It is also referred to as Chorioangiopagus parasiticus as the recipient twin is hemodynamically dependent on pump twin and thus acts as a parasite over it [1]. It receives blood from the pump twin via abnormal artery-to-artery or vein-to-vein communications on the surface of placenta. It is one of the types of twin to twin transfusion.
Normally umblical vein supplies oxygenated blood to the fetus and umblical artery takes back the deoxygenated blood away. But in TRAP sequence, there is an abnormal anastomosis between umblical arteries of the two monochorionic feti which causes the oxygenated blood to flow from pump twin to recipient twin and perfuses it and that is how the twin receives circulation even without a heart. There is a reversal of flow in umblical artery of acardiac twin, hence the name TRAP. This phenomenon can be demonstrated on Doppler study, which reveals reversed direction of spectral waveform in umblical artery of acardiac twin i.e. towards fetus (Figure 6). In 75% of cases, there can be associated single umblical artery in umblical cord of recipient twin [4].
The possible explanation behind the fetus having a better developed pelvis and lower extremities than head and thorax, as in our case, is that due to imbalanced circulation, the poor but relatively oxygenated blood from donor twin’s umblical artery flows in reversed direction into recipient’sumblical artery and from there-on into the lower body of fetus resulting into the lower body receivingrelatively more oxygen and nutrients than the upper torso. The de-saturated blood then flows in retrograde direction into the upper circulation i.e. the thorax, upper body and head resulting in mal-developed heart, head and upper torso, which are deformed or absent. This heterogeneous looking mass may simulate a teratoma on ultrasound scan [4].
There are two hypothesis regarding pathogenesis of TRAP sequence [5]
1. There is development of inherent deep placental anastomoses during early embryogenesis. Early pressure flow is more in one twin than that of the other, which leads to reversed perfusion in it. This causes malformation of acardiac twin [5].
2. Primary defect in embryogenesiswhich causes failure of heart development [5]. The perfusion of this twin is then maintained by artery-to-artery anastomoses with normal twin and the anastomoses not being responsible for cardiac anomaly.
Classification [5]
Schatz (1898) classified acardia into two groups:-
Hemiacardius- heart is formed imperfectly
Holoacardius- completely absent heart
Based on degree of cephalic and truncal mal-development, they can be classified as:-
Acardius acephalus: Cephalic structures (head and upper extremities) are absent. This is the most common form, accounting approximately two-thirds of the cases.
Acardius anceps: some cranial structure and neural tissue are present. Upper body and extremities are developed.
Acardius acormus: Cephalic structures present but truncal structures absent i.e Head without a body, cord is attached to head. It is the rarest form.
Acardius amorphous: No distinguishable cephalic or truncal structure noted. Only an amorphous mass is noted which simulates teratoma.
The present case was an Acardius Acephalus type wherein there was a malformed head and an absence of a bony cranium. Only a partially developed thorax, abdomen and lower body with flexed folded lower limbs were appreciated.
The pump twin is generally normal in structure; however in 10% of pump twins, congenital anomalies like cardiogenic defects, gastroschisis and skeletal abnormalities can develop [5]. There is also co-existence of VACTERL association found in surviving pump twin [6]. Polyhydramnios is generally associated since the pump twin is at high risk for developing anemia and heart failure as it is pumping for two. As a result there is an increased perfusion of fetal kidneys leading to overproduction of fetal urine and increased liquor consequently [7,8]. The perinatal mortality of pump twin is around 50-70%. It is either due to premature deliveryattributed to polyhydramnios or secondary to heart failure [4,7]. On Doppler study, difference in Resistive Index of umblical arteries of pump and acardiac twin more than 0.20 carries a good prognosis [4].
Since there is a high risk of perinatal complications, an early diagnosis and prompt intervention is needed to improve outcomes for pump twin. As a goal to protect the pump twin from bad outcome like prematurity and cardiac failure, various techniques have been proposed which are minimally invasive. The blood flow from pump twin to acardiac mass is interrupted by therapeutic interventions, thus reducing the hemodynamic overload on pump twin and eliminating the risk of cardiac failure and perinatal complications in it, resulting in better outcome. This is done under ultrasound guidance using a fetoscope [5]. Bipolar cord coagulation and Radiofrequency ablation are the two commonly used techniques [9]. The survival rate of pump twin after therapy with laser coagulation and RFA is 75-80% [10]. Others less commonly used techniques include cord occlusion by embolization, ligation, laser photocoagulation, alcohol injection, interstitial laser etc [5].
Although Invasive procedures are proposed to improve outcomes but they also carry an equal risk of procedure related pregnancy loss. Randomized control trials on timing to do interventional therapy are required [9]. Most recently, a novel non-invasive technique of High Frequency Ultrasound [HIFU] has been used which stops blood flow across vascular channels in TRAP but it also needs further development and research [9].
Conclusion
TRAP is a rarely encountered entity but comes with a poor prognosis when found. Accurate and early diagnosis can however lead to improved outcome to some extent. A radiologist should have a high index of suspicion while ultrasonographic scanning when encountered with a monochorionic twin pregnancy in which one twin continues to grow in spite of absence of heart or a heart like structure. The morphological features of the fetus on grey scale ultrasonography along with pathognomic Doppler findings aid in the early diagnosis of such a rare entity and warrant for clinically appropriate prenatal management. Such a clinical case scenario of TRAP sequence has been described through this report.
References
- Khanduri S, Chhabra S, Raja A, Bhagat S (2015) Twin reversed arterial perfusion sequence: a rare entity. J Clin Imaging Sci 5: 9.
- Buyukkaya A, Tekbas G, Buyukkaya R (2015) Twin Reversed Arterial Perfusion (TRAP) sequence; characteristic gray-scale and doppler ultrasonography findings. Iran J Radiol 12: e14979.
- Adamou N, Yakasai I (2014) Twin Reverse Arterial Perfusion (TRAP): Case report. Open J Obstet Gynecol 4: 1072-1076.
- Chandramouly M, Namitha (2009) Case series: TRAP sequence. Indian J Radiol Imaging 19: 81-83.
- Saritha S, Anjankar SS (2013) Twin Reversed Arterial Perfusion (TRAP) sequence. The Acardiac/Acephalic twin. Int J Anat Res 1: 140-144.
- Athwal S, Millard K, Lakhoo K (2010) Twin Reversed Arterial Perfusion (TRAP) sequence in association with VACTERL association: a case report. J Med Case Rep 4: 411.
- Ekşioğlu AS, Özgün A, Şenel S (2013) Twin Reversed Arterial Perfusion (TRAP) Sequence. Turkish J Pediatr Dis 1: 44-46.
- Prasad RHS, Prasad TR, Kumar KD (2012) TRAP sequence - An interesting entity in twins. J Clin Imaging Sci 2: 56.
- Aitken K, Andrews J, Mieghem TV, Windrim R, Kachura J, et al. (2014) Early Radiofrequency Ablation for Twin Reversed Arterial Perfusion (TRAP) sequence: Case report and literature review. Gynecol Obstet (Sunnyvale) 4: 239.
- Sommerfeldt JC, Putnins RE, Fung KFK, Grynspan D, Khaldoun Koujok K (2014) AIRP best cases in radiologic-pathologic correlation: twin reversed arterial perfusion sequence. RadioGraphics 34: 1385-1390.