Case Report
Early Diagnosis of Twin Interstitial Pregnancy Managed Conservatively: An Interesting and Rare Case Report
Ashwini G*, Samra Q and Badr SS
Department of Clinical Imaging, Women’s Hospital, Hamad Medical Corporation, Qatar
Corresponding author: Ashwini G, Department of Clinical Imaging, Women’s Hospital, Hamad Medical Corporation, Doha, Qatar, Tel no: 00974-33544845; E-mail: Agujrathi@hamad.qa
Citation: Ashwini G, Samra Q, Badr SS. Early Diagnosis of Twin Interstitial Pregnancy Managed Conservatively: An Interesting and Rare Case Report. Indian J Appl Radiol. 2018;4(1): 127.
Copyright ©2018 Ashwini G, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Indian Journal of Applied Radiology | Volume: 4, Issue: 1
Submission: 20/09/2018; Accepted: 03/11/2018; Published: 07/11/2018
Abstract
Interstitial ectopic pregnancies are quite uncommon. They accounts for 2-4% of all ectopic pregnancies. They have higher risks of rupture and hemorrhage compared to the usual tubal ectopic pregnancy. Hence an early diagnosis and timely management is imperative in preventing life-threatening morbidity and mortality. We report a very rare case of twin interstitial ectopic diagnosed early in our department and managed conservatively by methotrexate.
Keywords: Twin interstitial pregnancy; Ectopic; Ultrasound detection of ectopic pregnancy
Introduction
Interstitial ectopic pregnancy also known as intramural ectopic pregnancy is the implantation of the egg in the uterine horn. It is an exceptional entity that represents nearly 2-4% of all ectopic pregnancies [1]. Factors influencing the occurrence of interstitial twin pregnancy specifically and the true incidence are unknown because of the rarity of this condition [2]. Early diagnosis of interstitial pregnancy is a medical emergency because of the risk of rupture and death, the latter approaching 2.5% [3,4]. The interstitial or proximal portion of the fallopian tube lies within the muscular wall of the uterus. It is richly vascularized because it contains anastomoses between uterine and ovarian arteries [5]. Ultrasound studies and measurements of beta-human Chorionic Gonadotropin (hCG), which permit securing a diagnosis before interstitial rupture, have lowered the morbidity and mortality associated with ectopic pregnancies [4]. The treatment is typically surgical resection often radical by corneal resection or hysterectomy [6], although cases of medical treatment by methotrexate have been described. Conservative treatment allowed us to avoid surgical intervention and to preserve patient’s fertility [5]. We report a unique case of twin interstitial pregnancy detected by our department of women’s imaging on ultrasound and managed conservatively by systemic methotrexate.
Case Report
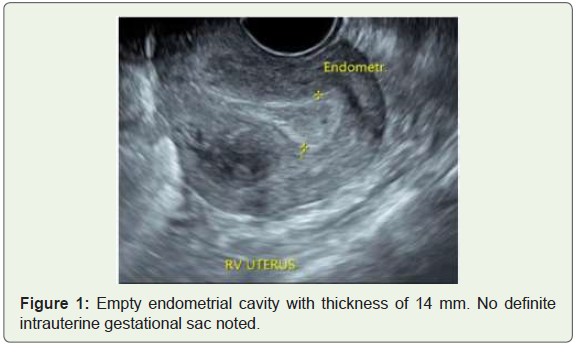
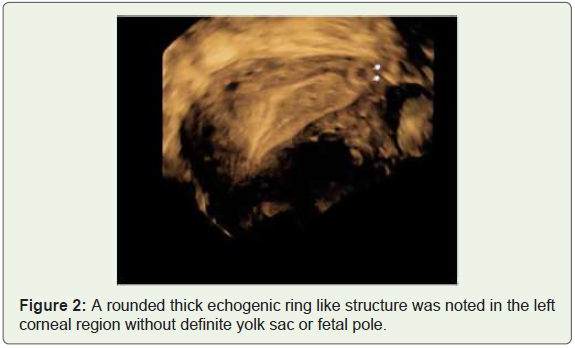
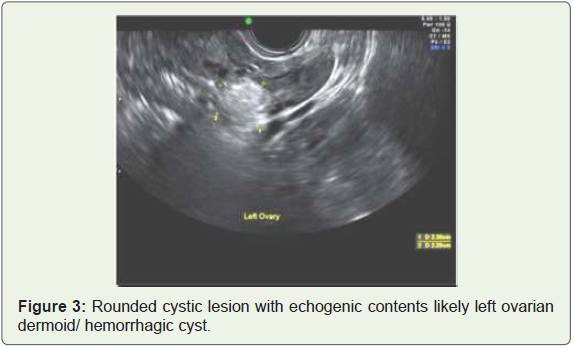
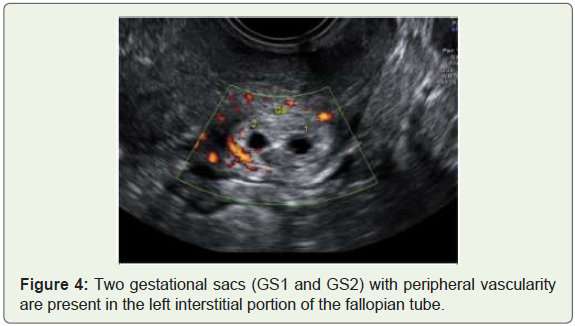
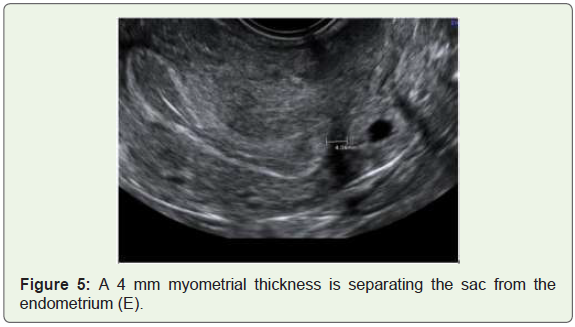
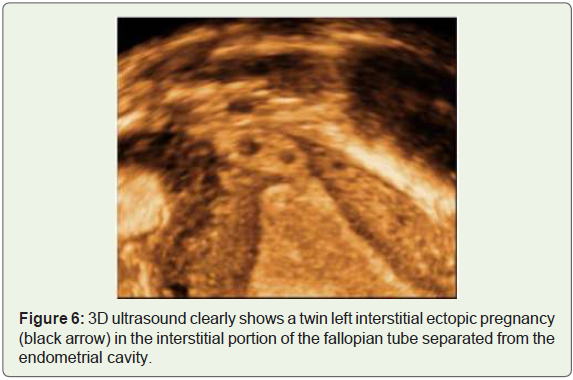
A 36 years multigravida, Gravida: 2, Para: 0; 7 weeks by LMP was referred to our Women’s emergency department as suspected ectopic pregnancy. Patient’s past medical history showed her as chronic hypertensive for 6 years on Aldomet (250mgs TID). Her Obstetric and gynecological history showed irregular periods on treatment for more than one year. History of one ectopic pregnancy 5 years back which was treated operatively with laparoscopic salpingectomy. The beta-hCG level was 1784 IU/ml and repeat beta-hCG was2029 IU/ml on the next day. On clinical examination patient was asymptomatic and hemodynamically stable. A transvaginal pelvic ultrasound was performed in our department and it showed an empty uterus with endometrial thickness of 14 mm (Figure 1). A rounded thick echogenic ring like structure was noted in the left corneal region without definite yolk sac or fetal pole with surrounding vascularity (Figure 2). A suggestion of left interstitial ectopic was made. There was a left ovarian dermoid cyst incidentally noted (Figure 3). Patient preferred conservative management with the hope of a chance for normal intrauterine pregnancy. It was planned to assess Beta-hCG, if normally doubling repeat ultrasound scan would be done and if plateau then methotrexate injection would be given. As beta-hCG doubled the next day, a repeat ultrasound was performed which showed two gestational sacs (Figure 4) in the left interstitial portion of the fallopian tube impressive of left twin interstitial pregnancy separated by 4 mm of myometrial thickness from the endometrial cavity (Figure 5). Patient decided to take conservative management with methotrexate and repeat serial beta-hCG. Patient remained asymptomatic and was discharged (Figure 6).
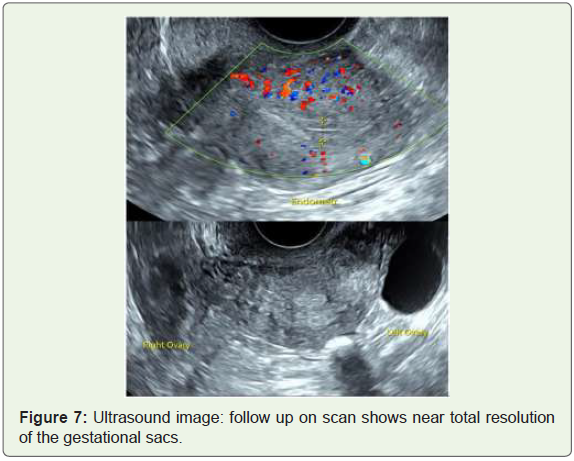
On follow up ultrasound, no residual lesion could be detected suggest complete resolution (Figure 7).
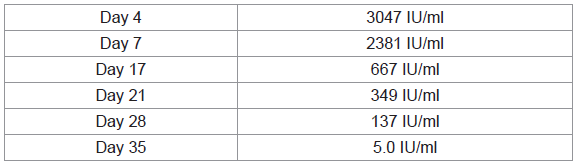
Following values of serial beta-hCG were taken (Table 1):
Discussion
Interstitial pregnancies are very rare and diagnosing them early in the gestation is imperative to avoid serious rupture and hemorrhage. It occurs within the interstitial portion of the fallopian tube with surrounding myometrium being quite distensible and therefore has the potential to grow to larger sizes than standard tubal ectopic pregnancies by the time of presentation [1].
The risk factors include advanced maternal age, IUD, tobacco, contraception micro progestin, endometriosis, history of pelvic surgery, recurrent pelvic inflammatory disease, uterine malformations and history of salpingectomy with cornual pregnancy on uterine stump [7].
The diagnosis of an interstitial pregnancy is quite challenging because it is difficult to distinguish it from an eccentric intrauterine pregnancy [3]. The diagnosis depends on the serial beta-hCG assays and imaging [5]. For many years, 2-D ultrasonography had a crucial role in early diagnosis of normal and ectopic pregnancy; nowadays, 3-D and 4-D ultrasound techniques allow highly accurate location of the gestational sac and describe its relations with the uterus and particularly with the myometrium [8]. Sonographic features that help in diagnosis include: an eccentric gestational sac; the diagnosis is suggested by visualization of an intrauterine gestational sac or decidual reaction located high in the fundus, with < 5 mm of surrounding myometrium in all planes. And an interstitial line sign; an echogenic line from the mass to the endometrial echo complex reportedly has high sensitivity (80%) and specificity (98%) [1]. MRI can also add to the ultrasound findings by showing presence of an intact junctional zone between the uterine cavity and the gestational sac surrounded by myometrium.
The management of interstitial pregnancy differs from the traditional cornual resection via laparotomy or even hysterectomy. Laparoscopic guided cornual wedge resection, cornuostomy and salpingectomy are recently tried and cause less surgical morbidity [3]. Conservative management with systemic methotrexate or local injection of potassium chloride is also applied [9]. Selective embolization has recently been proposed as an effective treatment. Recently Ultrasound guided transcervical evacuation under laparoscopic supervision has been described [7].
The complications include a recurrent ectopic and rupture in future pregnancies. Although successful vaginal deliveries after cornual resection have been reported, cesarean delivery is still advised to reduce the risk of rupture [3].
In conclusion, early diagnosis and timely management of an ectopic interstitial pregnancy is very crucial in preventing life-threatening damage. Different treatment options should be considered according to the clinical presentation. We detected an early twin interstitial pregnancy and patient was successfully treated conservatively.
MRI has been shown to be useful in the diagnosis of interstitial pregnancies as the presence of an intact junctional zone between the uterine cavity and the GS surrounded by myometrium is very suggestive of this condition. MRI may help differentiate an interstitial pregnancy from an angular pregnancy, when the embryo is implanted within the lateral angle of the uterine cavity medial to the uterotubal junction, or a pregnancy in a rudimentary horn (a true cornual pregnancy). In a clinically stable patient, MRI could provide more information and allow the consideration of conservative treatment.
References
- Knipe H, Gaillard F, et al. Interstitial Ectopic Pregnancy. rID: 1510.
- Casadio P, Formelli G, Spagnolo E, De Angelis D, Marra E, et al. (2009) Laparoscopic treatment of interstitial twin pregnancy. Fertil Steril 92: 390.e13-390.e17.
- Garretto D, Lee LN, Budorick NE, Figueroa R (2005) Interstitial twin pregnancy: A unique case presentation. J Clin Ultrasound 43: 447-450.
- Tulandi T, Al-Jaroudi D (2004) Interstitial pregnancy: results generated from The Society of Reproductive Surgeons Registry. Obstet Gynecol 103: 47-50.
- Cerviño E, Ramón Y, Cajal CL, Pérez P, Couceiro E (2011) Ultrasound-guided transcervical evacuation of interstitial twin pregnancy. Fertil Steril 96: 927-930.
- Mohamed B, Achour R, Nizar G, Samia BJ, Lotfi M, et al. (2012) A ruptured cornual ectopic pregnancy at 18 weeks’ gestation: A case report. The Internet J Gynaecol Obstet 16.
- Radhouane A, Jad D, Chadtha A, Adballah C, Monia M, et al. (2017) Cornual twin pregnancy: Diagnosis and management. Int J Sci Res 6.
- Douysset X, Verspyck E, Diguet A, Marpeau L, Chanauaz-Lachay I, et al. (2014) Grossesses interstitielles: traitement chirurgical, fertilité et devenir obstétrical. L’expérience rouennaise. Gynécologie Obstétrique & Fertilité 42: 216-221.
- Rastogi R, Gl M, Rastogi N, Rastogi V (2008) Interstitial ectopic pregnancy: A rare and difficult clinicosonographic diagnosis. J Hum Reprod Sci 1: 81-82.