Case Report
Multifocal Tumefactive Demyelination - Magnetic Resonance Imaging Features
Kumar K1* and Kumaran R2
1Associate Professor of Radio diagnosis, Velammal Medical College & Research Institute, India
2Assistant Professor of Radio diagnosis, Velammal Medical College & Research Institute, India
Corresponding author: Kumar K, Associate Professor of Radio diagnosis, Velammal Medical College & Research Institute, Madurai, Tamil Nadu-625009, India, Mobile: +91-9447345528; E-mail: drmkrishnakumar@gmail.com
Citation: Kumar K, Kumaran R. Multifocal Tumefactive Demyelination - Magnetic Resonance Imaging Features. Indian J Appl Radiol. 2018;4(1): 120.
Copyright © 2018 Kumar K, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Indian Journal of Applied Radiology | Volume: 4, Issue: 1
Submission: 26/09/2017; Accepted: 05/01/2018; Published: 10/01/2018
Abstract
Tumefactive Demyelinating Lesion (TDL), also referred as Monofocal Acute Inflammatory Demyelination (MAID), is a focal aggressive demyelination, usually manifesting as a solitary lesion or as few separate lesions greater than 2 cm that may mimic a tumor on neuro-imaging and pose a diagnostic challenge to the clinician as well as the radiologist.
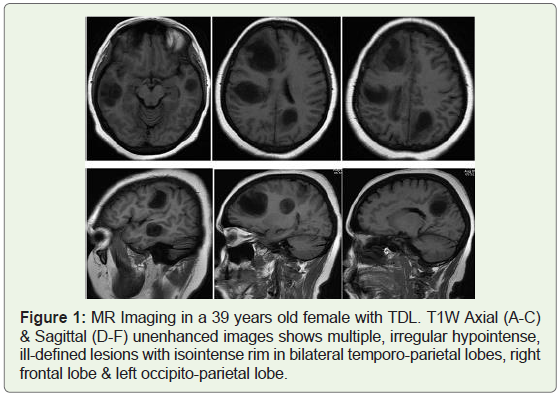
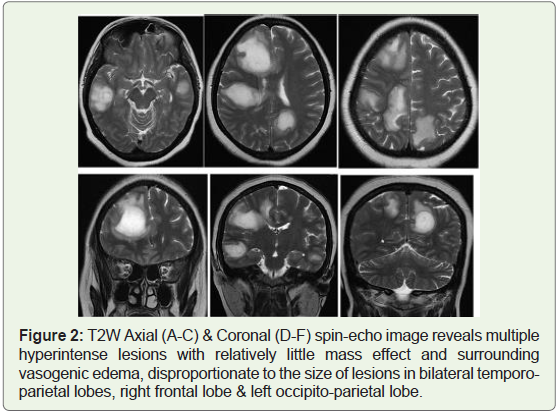
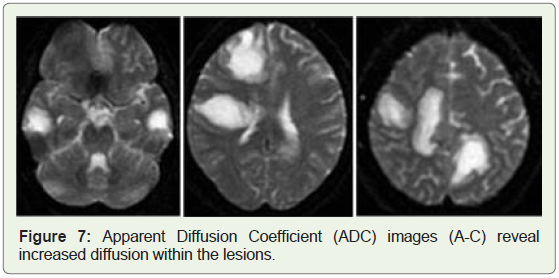
A precise diagnosis of TDL is absolutely essential as the management varies in TDL and Tumors. The magnetic resonance imaging (MRI) features suggestive of TDL include large white matter lesions with little mass effect or vasogenic edema, incomplete or open-ring enhancement, high central Apparent Diffusion Coefficients (ADC) and low relative Cerebral Blood Volume (rCBV). We report a 39 years old female patient presenting with gradual progression of weakness of left upper & lower limb followed by giddiness, headache & deviation of angle of mouth to right side, since 10 days, who had multifocal TDL mimicking metastatic brain tumor on imaging. The typical MRI features of the rare disease helped us to rule out tumor and spared the patient from invasive procedure such as biopsy and radiation from radiotherapy. Patient showed good improvement with corticosteroid therapy.
Keywords: ADEM; Glioma; Lymphoma; MRI; Multiple sclerosis; Tumefactive demyelination
Introduction
Primary demyelinating diseases of Central Nervous System (CNS) encompass several entities such as multiple sclerosis, myelinoclastic diffuse sclerosis and Acute Demyelinating Encephalomyelitis (ADEM) [1].
Tumefactive Demyelinating Lesions (TDLs) are defined as large (usually > 2 cm) demyelinating lesions mimicking brain tumors; they occur as solitary lesion or as a few separate lesions [2,3].
Clinical symptoms are atypical for Multiple Sclerosis (MS) and include focal neurologic deficit, seizure or aphasia. They can be found in 2.8% of MS patients or in patients without preexisting MS history, although they usually develop typical MS features in near future [4,5].
MRI is the most sensitive imaging technique for depicting demyelinating disease, but when a lesion manifests as a tumefactive lesion mimicking a tumor, especially glioma or CNS lymphoma, the correct diagnosis is often not made until after surgical biopsy or operation. Therefore, it appears that the differentiation of TDLs and these brain tumors by using MR imaging presents a diagnostic challenge.
Here we report a unique case of multifocal tumefactive demyelinating disease that was diagnosed with the help of MRI. The report has been approved by our Institutional Ethical committee.
Case Report
A39 years old female patient presenting with gradual progression of weakness of left upper & lower limb, followed by giddiness, headache & deviation of angle of mouth to right side, since 10 days, underwent contrast enhanced MRI ( GE Signa 1.5 Tesla) of brain, including multivoxel proton beam Spectroscopy.
Her blood pressure was 110/76 mm Hg. Laboratory investigation: Hemoglobin concentration: 11.8 g/dL, total leukocyte count: 7000/cu.mm with 65% neutrophils. Biochemical investigations: Random blood sugar, serum creatinine, sodium, potassium and calcium were within normal limits.
Serology for Human Immunodeficiency Virus (HIV), toxoplasmosis & Lyme disease was negative. Serum Aquaporin - 4 antibodies (NMOIgG) for neuromyelitis optica was negative. Cerebrospinal Fluid (CSF) analysis for Oligoclonal bands was negative for Multiple Sclerosis (MS). Stains & cultures for bacteria & mycobacteria were negative. Electroencephalogram was normal.
Neurological examination showed hypotonia with power of 3/5 in upper & lower limbs.
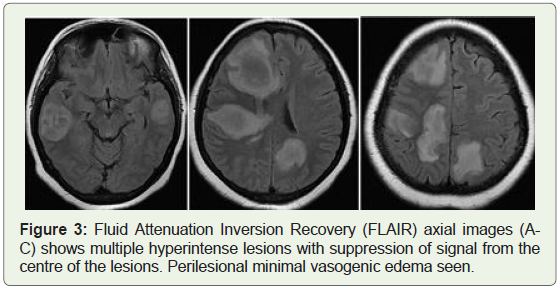
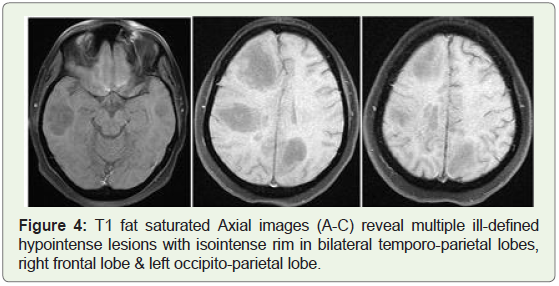
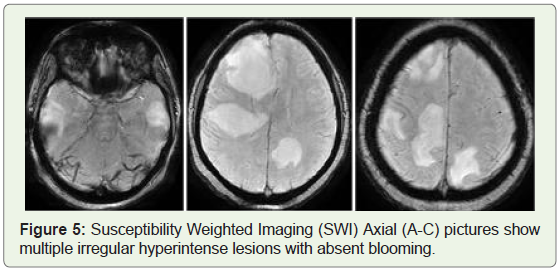
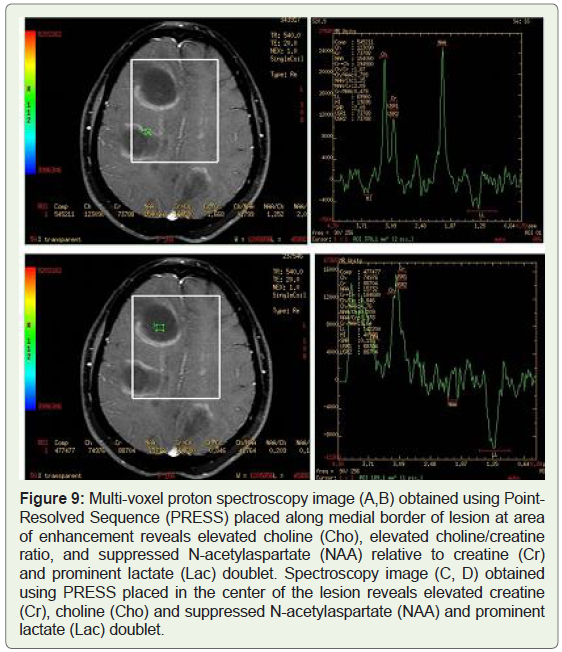
She was advised MRI for further evaluation. Routine T1W, T2W, FLAIR, T1W Fat sat, SWI, DWI, ADC and contrast enhanced T1W images in axial, coronal & sagittal planes were taken and images reviewed (Figures 1-8). Multi-voxel proton spectroscopy images were obtained using Point-Resolved Sequence (PRESS), placed along the medial border of the lesion at area of enhancement and centre of the lesion (Figure 9).
Our patient had no previous history of MS, presented with multiple brain lesions, mimicking metastatic brain disease which posed a serious diagnostic dilemma.
These typical clinical findings in an adult female with classical MRI findings, favoured the diagnosis of Tumefactive Demyelination. Progressive Multifocal Leukoencephalopathy (PML) was unlikely as the patient was not immune-compromised.
Discussion
The term Tumefactive Demyelinating Lesion (TDL) was first introduced by Kepes, et al. in 1993 [3]. In a review of 31 cases, Kepes proposed that tumefactive demyelinating lesions represent an intermediate lesion between those typically seen with multiple sclerosis and ADEM [3]. Tumefactive demyelination does not usually originate as a post-infectious or post-vaccination response.
The incidence of TDL has been reported to be 0.3 cases per 100,000 per year [6]. They occur more frequently in females especially during the second or third decade of life [7].
Usual clinical symptoms include headache, cognitive changes, mental confusion, aphasia and apraxia [4]. TDL is classically monophasic, most cases present with an upper motor neuron syndrome, although behavioral disorders, seizures and optic neuritis are also common manifestations. Symptoms in TDL are atypical for MS and are due to focal mass lesion leading to focal neurologic deficit, seizures and aphasia [8].
TDL can be isolated entity or presenting feature of MS (Tumefactive MS), pose a serious diagnostic challenge, to both clinicians and radiologists that frequently prompts biopsy in initial evaluation.
TDL often presents as large as, greater than 2 cm, enhancing lesions with mass effect and edema mimicking neoplasm, abscess or stroke [9]. The frontal lobe and parietal lobe are the most common locations of TDL and it presents as a single neurologic episode like in our case.
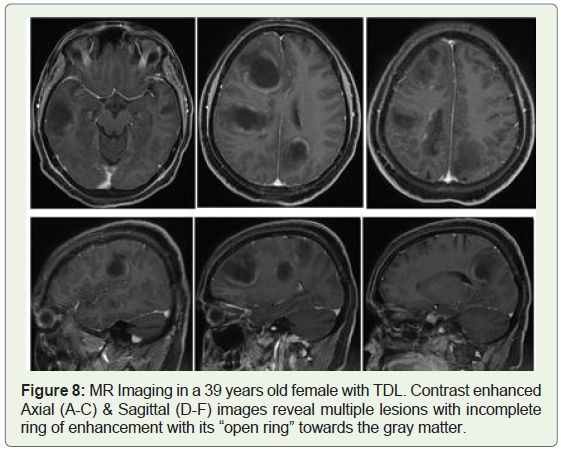
On MRI, TDL frequently demonstrate an incomplete arc of serpiginous ring enhancement that is more pronounced on the medial aspect of the lesions with the incomplete portion of the ring on the gray matter side of the lesion [10]. The enhancement corresponds to the areas of the most active demyelinating activity, with marked breakdown of the blood-brain barrier. This “open ring” pattern of enhancement differentiates ring-enhancing lesions caused by atypical demyelination from neoplasms or abscesses and has been reported in the literature as holding a degree of specificity for TDL [11-13].
Brain lymphoma, owing to its unifocal features and its good response to steroid therapy, is easily confused with TDL, but it shows marked homogeneous post contrast enhancement on T1W and isoor mild hyperintensity on T2-weighted images [12].
In contrast to TDL, neoplastic lesions more often show complete ring enhancement and greater mass effect, while abscesses show more extensive edema and central restriction on Diffusion-Weighted Imaging (DWI), as well as complete ring enhancement [4,5,14].
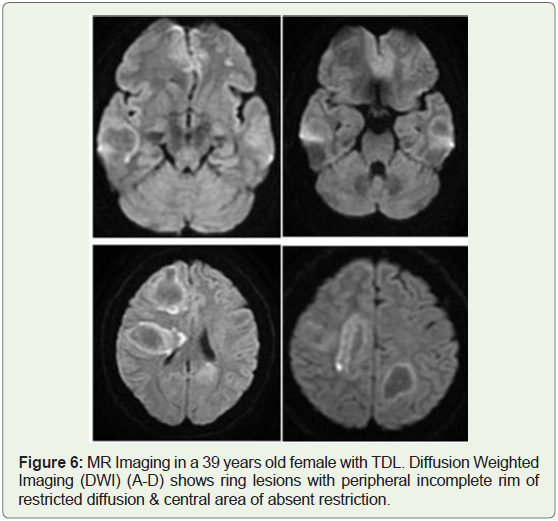
MRI characteristics, such as open-ring enhancement, peripheral restriction on diffusion-weighted imaging, or venular enhancement [9,14], location in the subcortical hemispheric white matter, relative lack of mass effect and perifocal edema may help to distinguish TDL from neoplastic lesions [15]. Follow up MR imaging may be used as a diagnostic aid to confirm the diagnosis, with interval improvement of these lesions following steroid therapy [15]. Further because many of the patients with TDL, develop definite MS (70%) most will have new lesions characteristic for time-space phenomenon of MS lesions on follow up imaging which may help to avoid biopsy [4,5,15] (Figure 6).
MR perfusion shows low Cerebral Blood Volume (rCBV) in demyelinating lesions in contrast to high rCBV in neoplastic lesions [14,16].
On MR Spectroscopy (MRS), elevated choline/creatine ratio, increased lactate, and normal N-acetylaspartate/creatine ratio may be regarded as suggestive of inflammation or demyelination [13,17]. Demonstration of elevation of the glutamate/glutamine peaks in MRI Spectroscopy is beneficial in the differential diagnosis of TDL because elevation of these peaks is not seen in neoplastic diseases of the brain [18].
On Diffusion Tensor Imaging (DTI), TDLs had a significantly higher incidence of intralesional hyperintensities on Fractional Anisotropy (FA) maps but a lower incidence of a perilesional hyperintense FA rim, compared with those of high-grade gliomas. In perilesional edema, FA values were significantly higher in high-grade gliomas [19].
On Computed Tomography (CT), attenuation of both MR enhancing and nonenhancing components of TDL was less than that of cortical and basal ganglia gray matter. CT hypoattenuation of MR enhanced regions is specific for distinguishing TDLs from primary glioma or CNS lymphoma and that the combined modalities of MR imaging and unenhanced CT are significantly more accurate than MR imaging alone for differentiating these entities [12].
A TDL misdiagnosed as a neoplasm could lead to unnecessary surgical intervention or even radiation therapy, which could exacerbate demyelinating diseases [20].
Positron Emission Tomography-Computed Tomography (PETCT) was used to evaluate metabolic activity of the suspected lesions. The TDL lesions revealed no pathologic metabolic activity, together with follow up MR helped to rule out focal brain as well as systemic neoplastic disease [21].
In rare cases, TDL may be associated with Hepatitis-C virus infection and HIV infection [22-24]. Hence HIV testing should be considered as part of the initial investigation of any patient who presents with focal brain syndrome with unusual “ring enhancement” on imaging.
The histopathologic characteristics of demyelinating lesions include the preservation of axons as shown by the presence of neurofilaments, the loss of myelin as shown by negative luxol fast blue staining, the presence of macrophages as shown by the presence of CD-68, and astrocytic proliferation as shown by the presence of glial fibrillary acidic protein [25].
Standard tumor histopathological protocols do not include staining with Luxol fast blue, which is used to detect myelination. Therefore, it is important for the clinician to have a high index of suspicion for a demyelinating lesion and relay this to the neuro-pathologist.
The therapeutic management includes Steroids, plasma exchange & Rituximab. If histological analysis is indicative of TDL, high-dose steroid treatment should be initiated, which can result in marked improvement in neurological deficits.MRS show normalization of initial increase in lipid & lactate peaks within 3-4 weeks, followed by persistent marked reduction of NAA levels.
In our case, diagnosis of TDL was made on the basis of clinical & typical MRI findings. With high dose intravenous corticosteroids (Methylprednisolone 1 g for 3-5 days) followed by oral tapering, patient showed good improvement in the focal deficit at the time of discharge and after 4 months follow up.
Conclusion
TDL prove to be a diagnostic dilemma to neurosurgeons, radiologists, and pathologists. In all cases, the characteristic MR imaging findings include mass lesions with “open-ring” enhancement. The MRI appearance of TDL, can aid in preoperative diagnosis and assist with the final pathologic interpretation, potentially sparing the patient from unnecessary brain biopsy and harmful therapies. With initiation of high-dose steroid treatment patients show marked improvement in neurological deficits.
References
- Xia L, Lin S, Wang ZC, Li SW, Xu L, et al. (2009) Tumefactive demyelinating lesions: Nine cases and a review of the literature. Neurosurg Rev 32: 171-179.
- Dagher AP, Smirniotopoulos J (1996) Tumefactive demyelinating lesions. Neuroradiology 38: 560-565.
- Kepes JJ (1993) Large focal tumor-like demyelinating lesions of the brain: intermediate entity between multiple sclerosis and acute disseminated encephalomyelitis? A study of 31 patients. Ann Neurol 33: 18-27.
- Lucchinetti CF, Gavrilova RH, Metz I, Parisi JE, Scheithauer BW, et al. (2008) Clinical and radiographic spectrum of pathologically confirmed tumefactive multiple sclerosis. Brain 131: 1759-1775.
- Altintas A, Petek B, Isik N, Terzi M, Bolukbasi F, et al. (2012) Clinical and radiological characteristics of tumefactive demyelinating lesions: follow-up study. Mult Scler 18: 1448-1453.
- Ragel BT, Fassett DR, Baringer JR, Browd SR, Dailey AT (2006) Decompressive hemicraniectomy for tumefactive demyelination with transtentorial herniation: Observation. Surg Neurol. 65: 582-583.
- Comi G (2004) Multiple sclerosis: Pseudotumoral forms. Neurol Sci 25: S374-S379.
- Paley RJ, Persing JA, Doctor A, Westwater JJ, Roberson JP, et al. (1989) Multiple sclerosis and brain tumor: a diagnostic challenge. J Emerg Med 7: 241-244.
- Javalkar V, Manix M, Wilson J, Nanda A (2012) Open ring enhancement in atypical brain demyelination. J Clin Neurosci 19: 910-912.
- Masdeu JC, Moreira J, Trasi S, Visintainer P, Cavaliere R, et al. (1996) The open ring: A new imaging sign in demyelinating disease. J Neuroimaging 6: 104-107.
- Masdeu JC, Quinto C, Olivera C, Tenner M, Leslie D, et al. (2000) Open-ring imaging sign: highly specific for atypical brain demyelination. Neurology 54: 1427-1433.
- Kim DS, Na DG, Kim KH, Kim JH, Kim E, et al. (2009) Distinguishing tumefactive demyelinating lesions from glioma or central nervous system lymphoma: added value of unenhanced CT compared with conventional contrast-enhanced MR imaging. Radiology 251: 467-475.
- Enzinger C, Strasser-Fuchs S, Ropele S, Kapeller P, Kleinert R, et al. (2005) Tumefactive demyelinating lesions: conventional and advanced magnetic resonance imaging. Mult Scler 11: 135-139.
- Jeong MS, Kim HS, Kim JH, Kim EK, Choi YS (2013) A Tumefactive multiple sclerosis lesion in the brain: an uncommon site with atypical magnetic resonance image findings. J Korean Soc Radiol 69: 337-341.
- Gavra M, Boviatsis E, Stavrinou LC, Sakas D (2011) Pitfalls in the diagnosis of a tumefactive demyelinating lesion: A case report. J Med Case Rep 5: 217.
- Neelima R, Krishnakumar K, Nair MD, Kesavadas C, Hingwala DR, et al. (2012) Tumefactive demyelinating lesions: a clinicopathological correlative study. Indian J Pathol Microbiol 55: 496-500.
- Koppula R, Degnan AJ, Ghassibi M, Duggan P, Jones R, et al. (2012) Neuroimaging of tumefactive multiple sclerosis with atypical features. Radiology Case Report 7: 1-5.
- Cianfoni A, Niku S, Imbesi SG (2007) Metabolite findings in tumefactive demyelinating lesions utilizing short echo time proton magnetic resonance spectroscopy. AJNR Am J Neuroradiol 28: 272-277.
- Toh CH, Wei KC, Ng SH, Wan YL, Castillo M, et al. (2012) Differentiation of tumefactive demyelinating lesions from high-grade gliomas with the use of diffusion tensor imaging. AJNR Am J Neuroradiol 33: 846-851.
- Peterson K, Rosenblum MK, Powers JM, Alvord E, Walker RW, et al. (1993) Effect of brain irradiation on demyelinating lesions. Neurology 43: 2105-2112.
- Dolic K, Bilic I, Buca A, Radovic D, Titlic M (2014) Differentiation of tumefactive demyelinating lesions from metastatic brain disease with fdg pet-ct: a case report. J Mult Scler 1: 108.
- Mestre TA, Correia de Sá J, Pimentel J (2007) Multifocal central and peripheral demyelination associated with hepatitis C virus infection. J Neurol 254: 1754–1756.
- Saravanan M, Turnbull IW (2009) Brain: non-infective and non-neoplastic manifestations of HIV. Br J Radiol 82: 956-965.
- Ball SC (2004) Rapid neurologic deterioration in a patient with HIV infection. AIDS Read 14: 63-66.
- Tan HM, Chan LL, Chuah KL, Goh NS, Tang KK (2004) Monophasic, solitary tumefactive demyelinating lesion: neuroimaging features and neuropathological diagnosis. Br J Radiol 77: 153-156.