Research Article
Assessment of Accuracy and Reliability of Linear Measurements of CBCT- An in vitro study
Sanjana R*, Poornima C, Mahesh Kumar TS, Balaji P and Mutreja D
Department of Oral Medicine and Radiology, Rajarajeswari Dental College and Hospital, Bengaluru, India
Corresponding author: Sanjana R, Post graduate student, Department of Oral Medicine and Radiology, Rajarajeswari Dental College and Hospital, Bengaluru, India; Tel: +91- 9480609591; Fax: 080-28437468; E-mail: sanjanaravindra@gmail.com
Citation: Sanjana R, Poornima C, Mahesh Kumar TS, Balaji P, Mutreja D. Assessment of Accuracy and Reliability of Linear Measurements of CBCT- An in vitro study. Indian J Appl Radiol. 2017;3(1): 119.
Copyright © 2017 Sanjana R, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Indian Journal of Applied Radiology | Volume: 3, Issue: 1
Submission: 17/10/2017; Accepted: 18/11/2017; Published: 20/11/2017
Abstract
Objectives: Cone Beam Computed Tomography (CBCT) is an innovative dental imaging system characterized by rapid volumetric imaging and allows us to obtain linear measurements in three dimensions using computer software. In order to optimize application of the technique in various fields it is necessary to analyse the accuracy of the data obtained on performing linear measurements. The present study intends to compare the linear measurements made on dry mandible with those made on CBCT images.
Method: The study consisted of 15 human dry mandibles. Sixteen linear measurements including 8 horizontal and 8 vertical, were made at different anatomical points of the dry mandible using Digital Vernier calliper. CBCT images were then obtained for the mandibles. The same linear measurements were done on the CBCT image using ONDEMAND 3D and Scanora softwares.
Results and Conclusion: Both the CBCT and the caliper measurements were highly reliable. The CBCT measurements tended to slightly underestimate the anatomic truth.
Keywords: Cone beam CT; Accuracy; Reliability; 3-D Imaging; Digital caliper
Introduction
Mah and Hatcher stated that- “If the aim is to improve the quality, efficiency and accessibility of craniofacial care, then there is a great need for accurate and effective imaging modalities” [1] . Thus, this study was undertaken to evaluate the accuracy of the linear measurements made on CBCT images.
Cone-beam Computed Tomography (CBCT) is a diagnostic tool that has revolutionized diagnosis and treatment planning in the dental field since 1995 [2]. Cone beam computed tomography is an image scanning and volumetric reconstruction technique that allows us to obtain linear measurements in three dimensions using computer software [3]. Though initially introduced in the field of dental implantology, CBCT has now made a place for itself in other fields like oral surgery, orthodontics, endodontics, periodontics, Temporomandibular Joint (TMJ) disorders, sleep apnea and in Ear, Nose and Throat (ENT) medicine [4,5]. Hence it becomes necessary to ascertain that the data obtained is accurate and reliable [6].
Materials and Method
The study group included 15 intact human dry mandible irrespective of age and gender. Five different anatomical points were chosen namely; Cd, Cr, Sc, Ma, Mf (Table 1). Based on these 5 anatomical landmarks, sixteen linear measurements (8 vertical and 8 horizontal) were made as depicted in Figures 1A-1C. The measurements were made on both sides of the jaw.
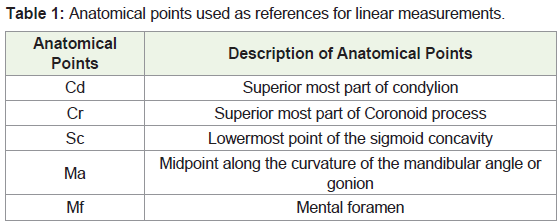
Table 1: Anatomical points used as references for linear measurements.
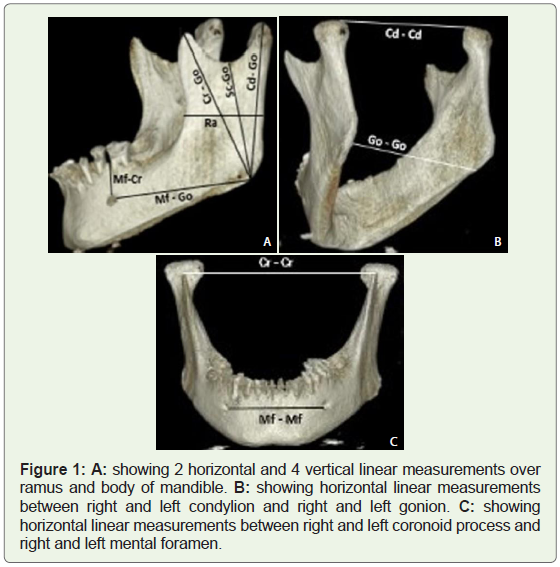
Figure 1: A: showing 2 horizontal and 4 vertical linear measurements over ramus and body of mandible. B: showing horizontal linear measurements between right and left condylion and right and left gonion. C: showing horizontal linear measurements between right and left coronoid process and right and left mental foramen.
The digital caliper measurements were considered the “gold standard” to which all CBCT measurements were compared. Measurements on the dry mandibular skulls were made by using a high-precision digital caliper Digimatic (Mitutoyo Corp, Kawasaki, Japan) which is calibrated to the nearest 0.01 mm.
Each mandible was scanned with the Scanora 3D CBCT Unit (Soredex, Finland) with CMOS Flat panel detector. The exposure parameters for the CBCT were as follows:- Field of view of 75 mm x 145 mm with a voxel size of 0.25 mm, 75 kVp, 13 mA and exposure time of 15 seconds. The ONDEMAND software was used for image processing and analysis. Images were viewed and analysed on a 24” DELL Flatron monitor (DELL, Precision T79110 XL, United States) with screen resolution of 1920 x 1200 pixels and 64- bit colour depth. Measurements on the scans were made with the computer program ONDEMAND. In the setting Volume Operation, the function “Measure Length” was used to measure distances on the 3D volumes. After marking 2 points (voxels) on the object of interest, the computer calculated the shortest distance between these points. Data were entered into an Excel 2013 spreadsheet (Microsoft).
All caliper and CBCT measurements (millimeter) were separately recorded by two independent trained observers. Each observer measured the distances using both digital caliper and ONDEMAND software, with calculation of the average of the distances obtained by the two observers with both methods. Intraoperator reliability was estimated by using the intraclass correlation coefficient. Reproducibility of measurements was assessed by repeating 80% of the measurements after a 2-weeks interval to eliminate memory bias.
The accuracy of the computer-generated measurements was assessed by comparing these measurements with the anatomic truth. Preliminary data analysis showed normal distribution for both samples, and the paired Student t test was used to determine statistically significant difference between the 2 groups. The level of significance was set at p<0.0025. Intraclass correlation coefficients were used to determine how well the 2 methods were correlated. All calculations were made with Statistical Package for the Social Sciences (SPSS) software (version 22).
Results
Comparison of the linear measurements made with digital caliper and CBCT showed no significant differences for 95% of the distances analysed [p>0.0025]. The intraclass correlation coefficient ranged from 0.981-1.000 mm in the measures analyzed using CBCT and from 0.997-1.000 mm in the measures obtained with the digital caliper, reflecting high reliability between the two observers.
The average discrepancy between the linear distances obtained with both methods ranged from 0.2 to 0.7 mm. Observer 1 did not report statistically significant differences for any of the 16 distances analysed while Observer 2 reported a statistically significant discrepancy for one of the 16 linear distances (Table 2). However, both the observers noted that CBCT underestimated the actual measurements in 15 of the 16 distances.
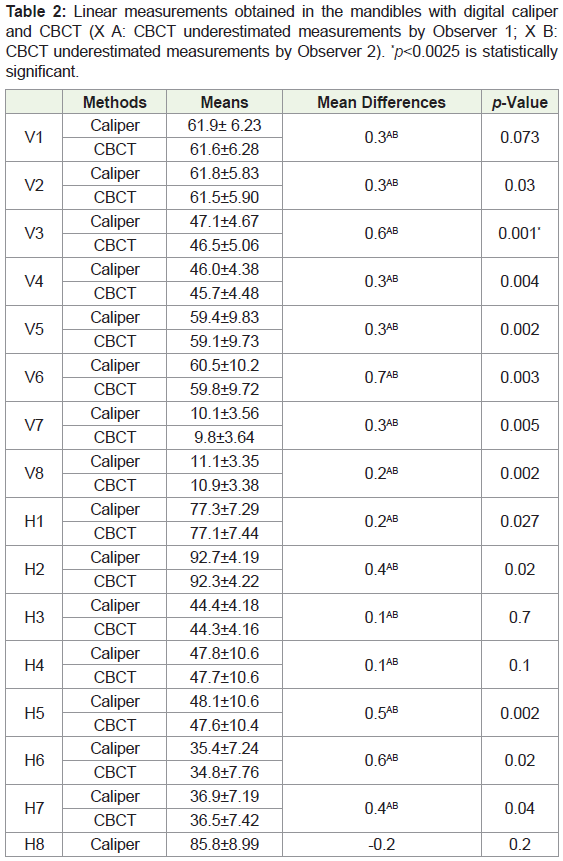
Table 2: Linear measurements obtained in the mandibles with digital caliper and CBCT (X A: CBCT underestimated measurements by Observer 1; X B: CBCT underestimated measurements by Observer 2). *p<0.0025 is statistically significant.
Discussion
A linear measurement assigns a numerical value for the length of an object or between objects. Human craniofacial dimensions were first analysed by anthropologists and anatomists who were based on osteolytic landmarks. With the invention of the x-ray machine, measurements were made on 2-Dimensional (2-D) diagnostic image rendered from a 3-Dimensional (3-D) structure [7,8].
All conventional two-dimensional (2-D) imaging procedures suffer from inherent limitations such as magnification, distortion, and superimposition leading to the misrepresentation of anatomic structures [9]. For these reasons, 3-D digital imaging systems have almost superseded 2-D analog imaging. Computed Tomography and CBCT represents a paradigm shift from two-dimensional (2-D) to three-dimensional (3-D) data acquisition and visualization.
Identification of anatomical structures, landmarks and accuracy of linear measurements is found to be superior in CBCT when compared to 2-D imaging [10,11]. Several studies have been undertaken to calibrate and test the accuracy of the quantitative measurements of the CT images. In various studies the accuracy of CT scans were found to be 1%, 0.28% with a range of 0.1% - 3.0 [12-14]. Linear measurements made on human mandible by axial CT demonstrated the accuracy which was within acceptable limits (0.4-0.9 mm) [15]. Hence, there is enough evidence to suggest that CT provides diagnostically accurate images.
Last decade has seen a significant upsurge in the manufacture, utility and availability of CBCT. Low radiation dose, sub millimeter spatial resolution, reduced scanning time and increasing access, have made CBCT a preferred imaging modality for the maxillofacial region. Hence, assessment of accuracy and reliability of CBCT imagesin terms of linear measurements gains significance.
Two hundred and forty linear measurements were made on human dry mandible, out of which 226 measurements [95%] showed no significant difference between digital caliper measurements and CBCT measurements. The observed minimum discrepancy of 5% being considered clinically acceptable. Average discrepancy demonstrated by our study was 0.2-0.7 mm which is similar to previous studies done by Brown et al. Waltrick et al. and Torres et al. with values 0.45 mm ± 0.17 mm, 0.23 mm ± 0.2 mm, 0.68 mm to 0.72 mm [16-18]. Studies done by Stratemann et al. Moreira et al. showed lesser average discrepancy than our study [19,20]. Kamburoglu et al. concluded that CBCT provides highly accurate data with less than 1% error when compared to physical measurements [21]. Most of the studies which compared CBCT to physical measurements found a tendency of CBCT to underestimate the anatomic truth [6,16-24]. Lascala et al. who showed that CBCT measurements for internal and external cranial anatomic sites tend to be slightly smaller than the same measurements made with caliper [5]. Underestimation wasrecorded on CBCT when synthetic mandible were used [22,23]. Hilgers et al. reported good accuracy and reliability of CBCT but Brown et al. concluded that 3-D CBCT data set using commercial analysis software have variable accuracy [16,24]. Baumgaertel et al. reported a systematic overestimation when analysis was performed [25].
Cone Beam Computed Tomography is known to produce 1:1 images as the magnification of these images are auto corrected [26]. The reasons for underestimation of linear measurements on CBCT images can be due to measurement software or partial volume effect [25]. The software defined the center of the volume from which to measure. In other words, the software might actually have measured the distance between the midpoints of the voxels. The caliper measures the distance between the contours of the skull, while the measurement software could have measured the distance between the centers of the mesial and distal voxel. For the field of view used in this study, the voxel size was 0.25 mm. If measurements were made from the center of the voxel, half of the voxel would not have been included in the measurement on either side (Figure 2). This would lead to CBCT measurements that are 0.25 mm smaller than caliper measurements. But all measurements were not necessarily 0.25 mm less in our study. Hence, this may not be the only reason for underestimation [27].
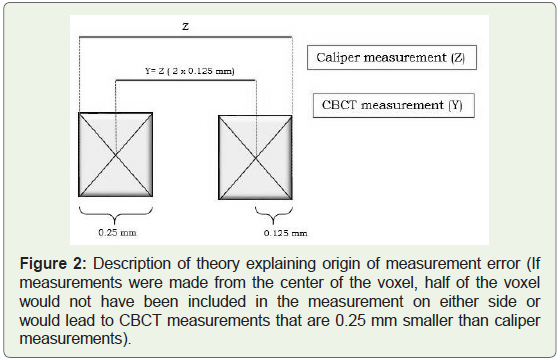
Figure 2: Description of theory explaining origin of measurement error (If measurements were made from the center of the voxel, half of the voxel would not have been included in the measurement on either side or would lead to CBCT measurements that are 0.25 mm smaller than caliper measurements).
A different theory termed “partial volume effect” could also explain our findings. According to this theory, if a voxel lies completely within an object, it would reflect that object’s density. However, if a voxel is at the junction of 2 objects of different densitieseg, bone and surrounding air-the voxel reflects an average value somewhere between the true values for bone and air (Figure 3) [27]. The ratio of bone to air in the voxel determines the voxel value. Such a “hybrid voxel” can be interpreted as part of the tooth or part of the surrounding air depending on the threshold value. High threshold values therefore create smaller than actual objects and vice versa.
Figure 3: Description of theory explaining the Partial volume effect (If a voxel lies completely within an object, it would reflect that object’s density. If a voxel is at the junction of 2 objects of different densities, the voxel reflects an average value).
The present study was designed to assess the reliability and accuracy of dental measurements made on CBCT images. Very few studies assessing the accuracy of CBCT measurements using dry skull have been documented in India. On reviewing the literature thoroughly, probably this is the first study made on Scanora 3D CBCT unit in comparing the linear measurements. One limitation of the present study is that no soft tissue or soft tissue equivalent was utilized so as to simulate a clinical situation. But using dry mandible could lead to better contrast in turn providing a higher level of accuracy.
Conclusion
The results of the study re-emphasize the fact that CBCT is an accurate and reliable measuring tool. Scanora 3D equipment like many other standard CBCT equipment also provides an accurate image. Hence CBCT images can therefore be used as an objective data that provides a near 1:1 accuracy of dimensional value.
References
- Berco M, Rigali PH Jr, Miner RM, DeLuca S, Anderson NK, et al. (2009) Accuracy and reliability of linear cephalometric measurements from cone-beam computed tomography scans of a dry human skull. Am J Orthod Dentofac Orthoped 136: 17.
- Tyndall DA, Rathore S (2008) Cone-beam CT diagnostic applications: Caries, periodontal bone assessment and endodontic applications. Dent Clin North Am 52: 825-841.
- Tarazona-Alvarez P, Romero-Millan J, Penarrocha-Oltra D, Fuster-Torres MA, Tarazona B, et al. (2014) Comparative study of mandibular linear measurements obtained by cone beam computed tomography and digital calipers. J Clin Exp Dent 6: e271-e274.
- Tetradis S, Anstey P, Graff-Radford S (2010) Cone beam computed tomography in the diagnosis of dental disease. J Calif Dent Assoc 38: 27-32.
- Zoller JE, Neugebauer J (2008) Fundamentals of Cone-beam Volumetric Imaging Technology. In: Cone-Beam volumetric imaging in dental, oral and maxillofacial medicine: Fundamentals, diagnostics and treatment planning. Quintessence Publishing, Chicago, IL, USA, pp. 214.
- Lascala CA, Panella J, Marques MM (2004) Analysis of the accuracy of linear measurements obtained by cone beam computed tomography (CBCT-NewTom). Dentomaxillofac Radiol 33: 291-294.
- Rubin RM (1997) Making sense of cephalometrics. Angle Orthod 67:83-85.
- Major PW, Johnson DE, Hesse KL, Glover KE (1994) Landmark identification error in posterior anterior cephalometrics. Angle Orthod 64: 447-454.
- Ganguly R, Ramesh A, Pagni S (2016) The accuracy of linear measurements of maxillary and mandibular edentulous sites in cone-beam computed tomography images with different fields of view and voxel sizes under simulated clinical conditions. Imaging Sci Dent 46: 93-101.
- Moshiri M, Scarfe WC, Hilgers ML, Scheetz JP, Silveira AM, et al. (2007) Accuracy of linear measurements from imaging plate and lateral cephalometric images derived from cone-beam computed tomography. Am J Orthod Dentofac Orthoped 132: 550-560.
- van Vlijmen OJ, Maal T, Bergre SJ, Bronkhorst EM, Katsaros C, et al. (2010) A comparison between 2D and 3D cephalometry on CBCT scans of human skulls. Int J oral Maxillofac surg 39: 156-160.
- Matteson SR, Bechtold W, Phillips C, Staab EV (1989) A method for three- dimensional image reformation for quantitative cephalometric analysis. J Oral Maxillofac Surg 47: 1053-1061.
- Hahn FJ, Chu WK, Cheung JY (1984) CT measurements of cranial growth: Normal subjects. AJR Am J Roentgenol 142: 1253-1255.
- Waitzman AA, Posmick JC, Armstrong DC, Pron GE (1992) Craniofacial skeletal measurements based on computed tomography: Part I. Accuracy and reliability. Cleft Palate Craniofac J 29: 112-117.
- Christiansen EL, Thompson JR, Kopp S (1986) Intra-and inter-observer variability and accuracy in the determination of linear and angular measurements in computed tomography: An in vitro and in situ study of human mandibles. Acta Odontol Scand 44: 221-229.
- Brown AA, Scarfe WC, Scheetz JP, Silveira AM, Farman AG (2009) Linear accuracy of cone beam CT derived 3D images. Angle Orthod 79: 150-157.
- Waltrick KB, Nunes de Abreu Junior MJ, Correa M, Zastrow MD, Dutra VD (2013) Accuracy of linear measurements and visibility of the mandibular canal of cone-beam computed tomography images with different voxel sizes: An in vitro study. J Periodontol 84: 68-77.
- Torres MG, Campos PS, Segundo NP, Navarro M, Crusoe-Rebello I (2012) Accuracy of linear measurements in cone beam computed tomography with different voxel sizes. Implant Dent 21: 150-155.
- Stratemann SA, Huang JC, Maki K, Miller AJ, Hatcher DC (2008) Comparison of cone beam computed tomography imaging with physical measures. Dentomaxillofac Radiol 37: 80-93.
- Moreira CR, Sales MA, Lopes PM, Cavalcanti MG (2009) Assessment of linear and angular measurements on three-dimensional cone-beam computed tomographic images. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 108: 430-436.
- Kamburoglu K, Kolsuz E, Kurt H, Kilic C, Ozen T, et al. (2011) Accuracy of CBCT measurements of a human skull. J Digit Imaging 24: 787-793.
- Damstra J, Fourie Z, Huddleston Slater JJ, Ren Y (2010) Accuracy of linear measurements from cone-beam computed tomography-derived surface models of different voxel sizes. Am J Orthod Dentofacial Orthop 137: 1-17.
- Lagravere MO, Carey J, Toogood RW, Major PW (2008) Three-dimensional accuracy of measurements made with software on cone-beam computed tomography images. Am J Orthod Dentofacial Orthop 134: 112-116.
- Hilgers ML, Scarfe WC, Scheetz JP, Farman AG (2005) Accuracy of linear temporomandibular joint measurements with cone beam computed tomography and digital cephalometric radiography. Am J Orthod Dentofacial Orthop 128: 803-811.
- Baumgaertel S, Palomo JM, Palomo L, Hans MG (2009) Reliability and accuracy of cone-beam computed tomography dental measurements. Am J Orthod Dentofacial Orthop 136: 19-25.
- Alamri HM, Sadrameli M, Alshalhoob MA, Sadrameli M, Alshehri MA (2012) Applications of CBCT in dental practice: A review of the literature. Gen Dent 60: 390-400.
- Schultz E, Felix R, Lackner K, Bergeder HD, Thurn P (1979) Image characteristics of the computer tomograph. RoFo 130: 479-486.