Case Report
Cephalothoracopagus: A Rare Congenital Anomaly
Ashwini S Gujrathi1, Sanaa Syed Badr Ahmed1, Reda Ramadan Yousef1, Wojciech Szmigielski2
1Department of Clinical Imaging, Women’s Hospital, Hamad Medical Corporation, Doha, Qatar
2Department of Clinical Imaging, National Center for Cancer Care and Research, Hamad Medical Corporation,Doha, Qatar
Corresponding author: Wojciech Szmigielski, Department of Clinical Imaging, National Center for Cancer Care and Research, Hamad Medical Corporation, P.O. Box 3050, Doha, Qatar; E-mail: w.szmigielski@gmail.com; wszmigielski@hamad.qa
Citation: Ashwini G, Badr Ahmed SS, Yousef RR, Szmigielski W. Cephalothoracopagus: A Rare Congenital Anomaly. Indian J Appl Radiol. 2017;3(1): 117.
Copyright © 2017 Ashwini G, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Indian Journal of Applied Radiology | Volume: 3, Issue: 1
Submission: 10/11/2017; Accepted: 20/11/2017; Published: 22/11/2017
Abstract
Conjoined twins are rarely seen congenital anomaly. Conjoined twins develop when there is cleavage in to embryos occurs on day 13 or later. There are wide variety of conjoined twins depending on which part of body are connected .It is associated with severe mortality and morbidity. The most common types of conjoined twins include the thoracopagus type where the fusion is anterior at the chest.
Method: We are reporting two cases of conjoined thoracopagus twins diagnosed by ultrasonography at 28 weeks and at 12 weeks. Because this situation carries high risk, early diagnosis and management of delivery is extremely important. The role of ultrasound in early diagnosis is discussed.
Conclusions: Ultrasound plays an important role in the diagnosis of this congenital anomaly. It provides findings that allow establishing the type and severity of the abnormality.
Keywords: Pregnancy complication; Congenital fetal anomaly; Twins conjoined
Background
Conjoined twins represent one of the rarest forms of twin gestation. They occur in roughly 1 in every 200 identical twin pregnancies and are always identical. The incidence ranges from 1 in 50 000 to 1 in 100 000 live births. The most common types of conjoined twins include the thoracopagus type, where the fusion is anterior, at the chest. This gestational anomaly is associated with severe mortality and morbidity. Therefore, early diagnosis and management of delivery is extremely important. The role of ultrasound in early diagnosis and management is discussed.
We report two cases of conjoined cephalothoracopagus twins diagnosed by ultrasonography at 28 weeks and at 12 weeks.
Two Cases Report
Case 1
A 39 year old lady G2P1, LSCS lower segment Cesarean Section. The patient was presented to our emergency department with abdominal pain. There was history of decreased fetal movements. The patient did not have any ANC antenatal care; no previous ultrasound scan was available. Clinically polyhydramnios was suspected due to increased uterine fundal height for gestational age. The ultrasound examination at 28 weeks revealed: Two separate pelvises with urinary bladders (Figure 1A-D). There was presence of polyhydramnios, with deepest pocket measuring 12.0 cm. Two beating fetal hearts in one thoracic cavity and two separate spines were identified. Two fetal heads joined at temporoparietal area were identified.
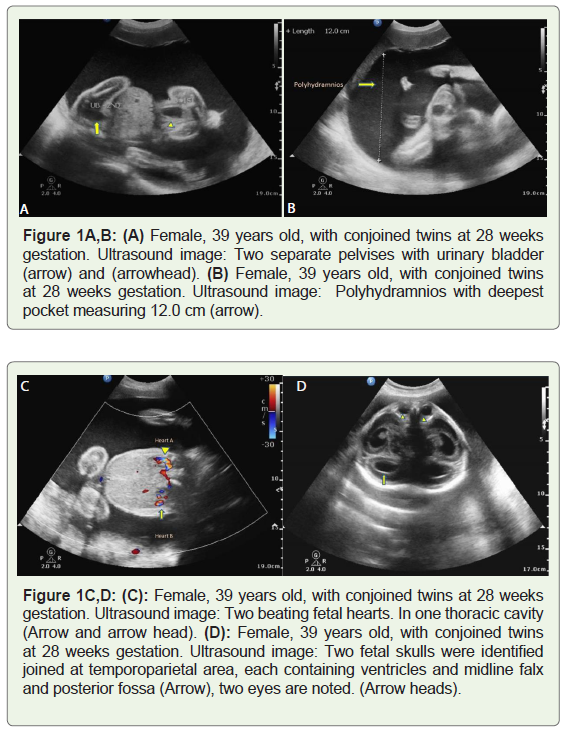
Figure 1A-D: (A) Female, 39 years old, with conjoined twins at 28 weeks gestation. Ultrasound image: Two separate pelvises with urinary bladder (arrow) and (arrowhead). (B) Female, 39 years old, with conjoined twins at 28 weeks gestation. Ultrasound image: Polyhydramnios with deepest pocket measuring 12.0 cm (arrow). (C): Female, 39 years old, with conjoined twins at 28 weeks gestation. Ultrasound image: Two beating fetal hearts. In one thoracic cavity (Arrow and arrow head). (D): Female, 39 years old, with conjoined twins at 28 weeks gestation. Ultrasound image: Two fetal skulls were identified joined at temporoparietal area, each containing ventricles and midline falx and posterior fossa (Arrow), two eyes are noted. (Arrow heads).
Both were demonstrating lateral cerebral ventricles and midline falx cerebri as well as posterior fossa structures. One fetal face was identified , one nose , two eyes and one mouth. Two upper limbs and four lower limbs were identified. On the basis of these findings the diagnosis of JENICEPS was made.
Case 2
A 32 was referred to our department, Women’s Hospital for (NT) Nuchal Translucency scan at 12-weeks gestation. She had no personal or family history of twins. Ultrasonography revealed two fetuses with two arms and two legs. A single head was demonstrated. The twins were joined at the thoraces and upper abdomens. There was a single umbilical cord with one artery and two veins. Two beating fetal hearts were observed (Figure 2A). The placenta was localized anteriorly. On the basis of these findings, the diagnosis of thoracopagus, conjoined twins was made (Figure 2B). The patient was informed about the malformation found and the twins’s poor chance for survival. The parents decided to terminate the pregnancy in their own country. [1,2] (Figure 2C,D).
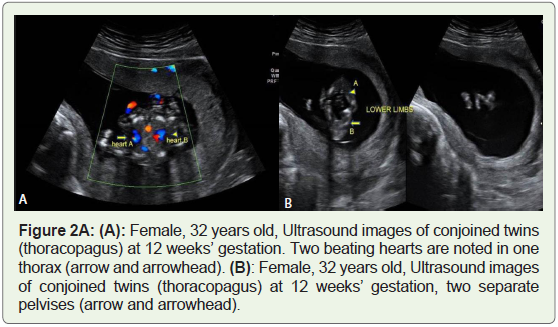
Figure 2A: Female, 32 years old, Ultrasound images of conjoined twins (thoracopagus) at 12 weeks’ gestation. Two beating hearts are noted in one thorax (arrow and arrowhead).
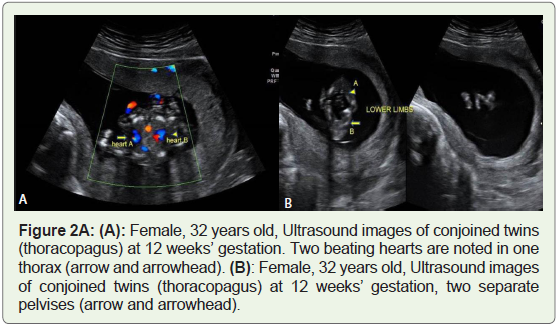
Figure 2B: Female, 32 years old, Ultrasound images of conjoined twins (thoracopagus) at 12 weeks’ gestation, two separate pelvises (arrow and arrowhead).
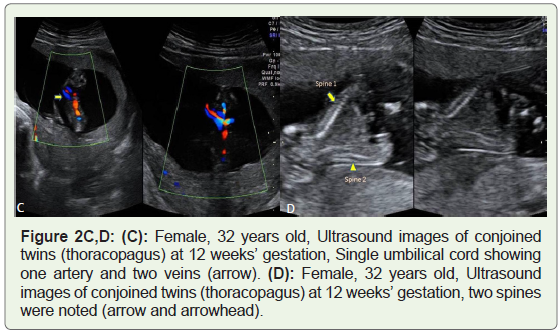
Figure 2C,D: (C): Female, 32 years old, Ultrasound images of conjoined twins (thoracopagus) at 12 weeks’ gestation, Single umbilical cord showing one artery and two veins (arrow). (D): Female, 32 years old, Ultrasound images of conjoined twins (thoracopagus) at 12 weeks’ gestation, two spines were noted (arrow and arrowhead).
Discussion
Conjoined twins are classified according to the most prominent site of conjunction: thorax (thoracopagus), abdomen (omphalopagus), sacrum (pygopagus), pelvis (ischiopagus), skull (cephalopagus) and back (rachipagus).
Depending on the aspect of the embryonic disc, the most common types are thoracopagus (19%) [3] (Table 1). Its etiology is unknown, but an incomplete division of the zygote between 13th and 15th days after fertilization probably occurs [4]. The overall survival rate for conjoined twins is approximately 25% [5]. The condition is more frequently found among females, with a ratio of 3: 1 [4]. Two theories have been proposed to explain this observation: the process of X-inactivation overlaps with the timing of monozygotic twinning and thus may directly contribute to development of monozygotic twins, and the XX karyotype may confer a survival benefit [2] (Figure 2E,F).
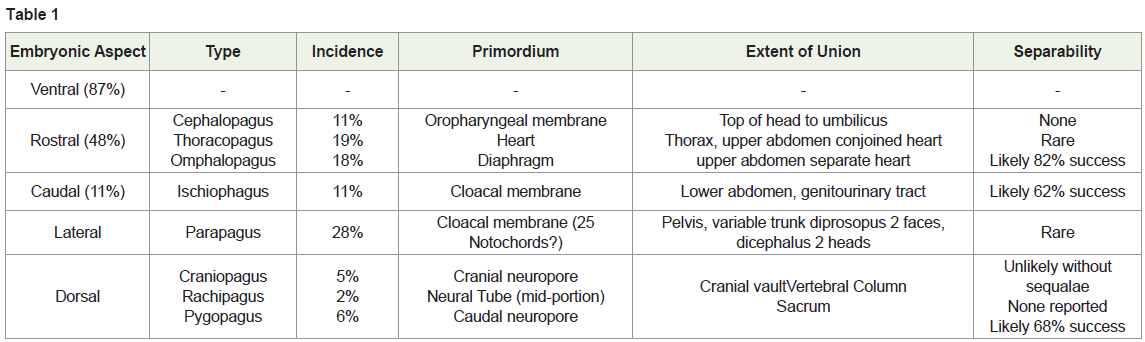
Table 1
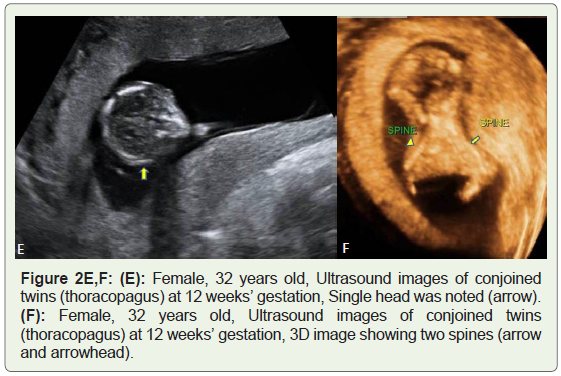
Figure 2E,F: (E): Female, 32 years old, Ultrasound images of conjoined twins (thoracopagus) at 12 weeks’ gestation, Single head was noted (arrow). (F): Female, 32 years old, Ultrasound images of conjoined twins (thoracopagus) at 12 weeks’ gestation, 3D image showing two spines (arrow and arrowhead).
Embryologic classification of conjoined.
Two contradicting theories exist to explain the origins of conjoined twins. The traditional theory is fission, in which the fertilized egg splits partially and conjoined twins represent delayed separation of the embryonic mass after day 12 of fertilization. The second theory is fusion, in which a fertilized egg completely separates, but stem cells (which search for similar cells) find like-stem cells on the other twin and fuse the twins together [4,6,7]. Conjoined twins share a single common chorion, placenta, and amniotic sac, although these characteristics are not exclusive to conjoined twins as there are some monozygotic but nonconjoined twins that also share these structures in utero [4,6] (Figure 2G-I).
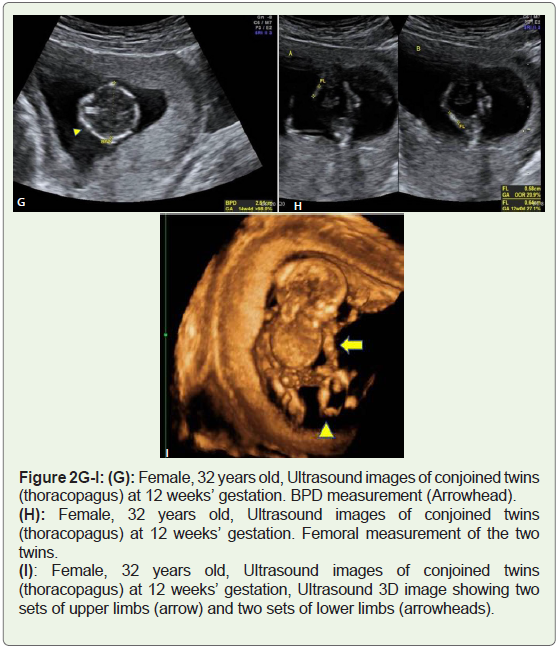
Figure 2G-I: : (G): Female, 32 years old, Ultrasound images of conjoined twins (thoracopagus) at 12 weeks’ gestation. BPD measurement (Arrowhead).(H): Female, 32 years old, Ultrasound images of conjoined twins (thoracopagus) at 12 weeks’ gestation. Femoral measurement of the two twins.(I): Female, 32 years old, Ultrasound images of conjoined twins (thoracopagus) at 12 weeks’ gestation, Ultrasound 3D image showing two sets of upper limbs (arrow) and two sets of lower limbs (arrowheads).
Early diagnosis of conjoined twins was previously reported, but not before the 10th week of gestation [8]. On careful transvaginal sonography and serial scanning, there appears to be an inability to separate between the anatomical parts of the fetuses. Once conjoined twins have been diagnosed, characterization of the type and severity of the abnormality can be performed with ultrasound, three-dimensional ultrasound, computed tomography, or magnetic resonance imaging [9,10]. Termination of pregnancy can be offered to the family. In the present study, the diagnosis has been performed in the first trimester, and because the family has chosen termination of this pregnancy, further diagnostic intervention has not been considered. Surgery to separate conjoined twins may range from relatively simple to extremely complex, depending on the point of attachment and the internal parts that are shared. Most cases of separation are extremely risky and life-threatening (Figure 3).
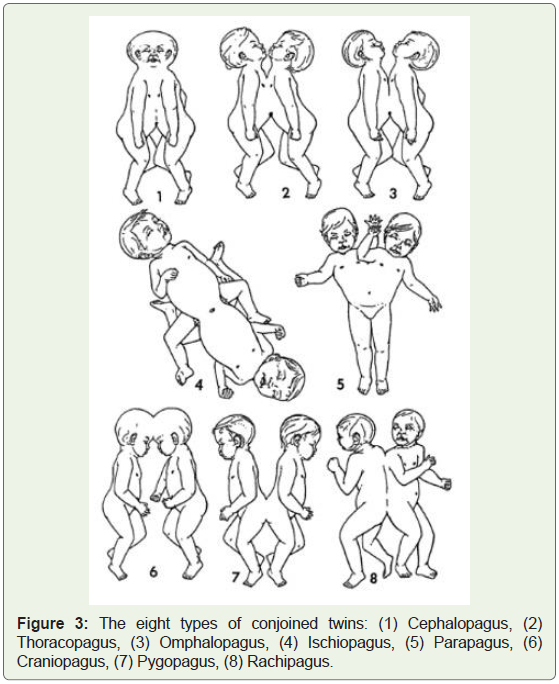
Figure 3: The eight types of conjoined twins: (1) Cephalopagus, (2) Thoracopagus, (3) Omphalopagus, (4) Ischiopagus, (5) Parapagus, (6) Craniopagus, (7) Pygopagus, (8) Rachipagus.
Conclusion
Ultrasound plays an important role in the diagnosis of this congenital anomaly. It provides findings that allow establishing the type and severity of the abnormality. Conjoined twins are associated with a high perinatal mortality; therefore, making an early diagnosis gives the parents a chance to elect pregnancy termination.
References
- Rees AEJ, Vujanic GM, Williams WM (1993) Epidemic of conjoined twins in Cardiff. BJOG 100: 388-391.
- Chitnis S, Derom C, Vlietinck R, Derom R, Monteiro J, et al. (1999) X chromosome-inactivation patterns confirm the late timing of monoamniotic-MZ twimming. Am J Hum Genet 65: 570-571.
- Schnaufer L (1980) Conjoined twins. In: Raffensperger JG, [Eds]. Swenson’s Pediatric Surgery (4th eds) New York, NY, USA: Appleton Century-Crofts Pp:910-920.
- Abossolo T, Dancoisne P, Tuaillon J, Orvain E, Sommer JC, et al. (1994) Early prenatal diagnosis of asymmetric cephalothoracopagus twins. J Gynecol Obstet Biol Reprod (Paris) 23: 79-84.
- Stone JL, Goodrich JT (2006) The craniopagus malformation: classification and implications for surgical separation. Brain 129: 1084-1095.
- Spencer R (2000) Theoretical and analytical embryology of conjoined twins: part I: embryogenesis. Clin Anat 13: 36-53.
- Spencer R (2000) Theoretical and analytical embryology of conjoined twins: part II: adjustments to union. Clin Anat 13: 97-120.
- Hubinont C, Kollmann P, Malvaux V, Donnez J, Bernard P (1997) First-trimester diagnosis of conjoined twins. Fetal Diagn Ther 12: 185-187.
- Kuroda K, Kamei Y, Kozuma S, Kikuchi A, Fujii T, et al. (2000) Prenatal evaluation of cephalopagus conjoined twins by means of three-dimensional ultrasound at 13 weeks of pregnancy. Ultrasound Obstet Gynecol 16: 264-266.
- Kingston CA, McHugh K, Kumaradevan J, Kiely EM, Spitz L (2001) Imaging in the preoperative assessment of conjoined twins. Radiographics 21: 1187-1208.