Case Report
Multicentric Urothelial Cell Carcinoma Involving Renal Pelvis, Ureter, and Vesicoureteric Junction: A Case Report
Sneha Tapashetti*, Vidhya Rani R, Annamaneni Chandrahas and Sandhya R
Department of Radiodiagnosis, Sapthagiri Institute of medical Science and Research Centre, Bangalore, Karnataka, India
*Corresponding author:Sneha Tapashetti, Department of Radiodiagnosis, Sapthagiri Institute of medical Science and Research Centre, Bangalore, Karnataka, India. E-mail Id: snehatapashetti@gmail.com
Copyright: © 2026 Tapashetti S, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article Information:Submission: 16/02/2026; Accepted: 26/03/2026; Published: 31/03/2026
Abstract
Background: Urothelial carcinoma (UC), previously termed transitional cell carcinoma, is an uncommon but aggressive malignancy arising from the urothelium of the renal pelvis and ureter. It is characterized by a high propensity for multifocality, local invasion, and distant metastasis. Synchronous
multicentric involvement extending from the renal pelvis to the ureter and vesicoureteric junction is rare and reflects a pan-urothelial field change, posing diagnostic and therapeutic challenges.
Case Presentation: We report the case of a 60-year-old female who presented with intermittent, colicky left loin pain of six months’ duration, without hematuria or constitutional symptoms. Contrast-enhanced computed tomography revealed a large hypoenhancing mass arising from the left renal pelvis
with frond-like intraluminal calyceal extensions, severe pelvicalyceal dilatation, marked cortical thinning, and encasement of the left renal artery with renal vein involvement. Tumor extension was noted into the proximal and mid ureter, along with a separate lesion at the left vesicoureteric junction producing an
intravesical filling defect. Enlarged left renal hilar lymph nodes and multiple hepatic lesions were identified. FDG PET-CT demonstrated metabolically active disease involving the renal pelvis, ureter, vesicoureteric junction, renal vein, and liver, consistent with multicentric metastatic UC. The patient underwent
biopsy and histopathological examination confirmed urothelial cell carcinoma.
Conclusion: This case highlights the aggressive behavior and multicentric nature of UC, emphasizing the importance of comprehensive imaging for accurate staging. Recognition of synchronous pan-urothelial involvement is crucial, as it is associated with advanced disease, poorer prognosis, and the
need for radical management with close oncologic surveillance.
Keywords:Urothelial carcinoma; Renal pelvis tumor; Multicentric urothelial carcinoma; CT urography; FDG PET-CT
Introduction
Transitional cell carcinoma (TCC), also referred to as urothelial
carcinoma, is the most common malignancy of the urinary tract,
predominantly arising in the urinary bladder [1]. Tumors originating
in the upper urinary tract, including the renal pelvis and ureter,
are relatively uncommon and account for approximately 5-10% of
all urothelial neoplasms. Despite their lower incidence, upper tract
TCCs are clinically significant due to their aggressive biological
behavior, diagnostic challenges, and high propensity for multifocality
and recurrence [2].
Upper tract TCC most frequently presents in the sixth and seventh
decades of life, with a marked male predominance. Established risk
factors include cigarette smoking, exposure to aromatic amines,
chronic analgesic abuse, cyclophosphamide therapy, and endemic
nephropathies such as Balkan nephropathy [3]. These carcinogens are
excreted in urine, leading to prolonged contact with the urothelium
and resulting in a field cancerization effect, which explains the
frequent occurrence of synchronous and metachronous tumors
throughout the urothelial lining [4].
A hallmark feature of urothelial carcinoma is its multicentric
nature. Multifocal involvement of the renal pelvis and ureter is well
documented; however, continuous involvement extending to the
midureter is distinctly rare. Such extensive disease supports the theory
of pan-urothelial susceptibility, wherein genetically altered urothelial
cells give rise to tumors at multiple sites simultaneously. Multicentric
disease has been associated with higher tumor grade, advanced stage
at presentation, and poorer overall prognosis compared to solitary
lesions [5].
Clinically, patients most commonly present with painless gross or microscopic hematuria. Flank pain may occur secondary to obstruction, while lower urinary tract symptoms can be present when distal ureteric or vesicoureteric junction involvement exists. Due to the retroperitoneal location of the upper urinary tract, tumors may remain clinically silent until significant obstruction or renal impairment develops, often leading to delayed diagnosis [6].
In bladder urothelial cancers that are usually identified through direct cystoscopic visualization, tumors in the upper urinary tract depend primarily on radiologic techniques for their identification, evaluation, and determination of disease extent. [1]
Radiological imaging plays a pivotal role in the detection and staging of upper tract UC. Multiphasic computed tomography urography has emerged as the imaging modality of choice, allowing comprehensive evaluation of the renal parenchyma, collecting system, ureter, and surrounding structures in a single examination. Typical imaging features include filling defects, focal wall thickening, infiltrative growth patterns with preservation of renal contour, and extension along the urothelial surface. Accurate imaging assessment is essential for differentiating UC from other centrally located renal masses and for determining the extent of multicentric involvement [7].
Management of upper tract UC depends on tumor grade, stage, and extent of disease. Radical nephroureterectomy with bladder cuff excision remains the gold standard for high-risk or multifocal tumors. The presence of multicentric disease involving the renal pelvis, ureter, and vesicoureteric junction underscores the need for meticulous surgical planning and long-term surveillance, given the high risk of recurrence and subsequent bladder involvement [8]
Clinically, patients most commonly present with painless gross or microscopic hematuria. Flank pain may occur secondary to obstruction, while lower urinary tract symptoms can be present when distal ureteric or vesicoureteric junction involvement exists. Due to the retroperitoneal location of the upper urinary tract, tumors may remain clinically silent until significant obstruction or renal impairment develops, often leading to delayed diagnosis [6].
In bladder urothelial cancers that are usually identified through direct cystoscopic visualization, tumors in the upper urinary tract depend primarily on radiologic techniques for their identification, evaluation, and determination of disease extent. [1]
Radiological imaging plays a pivotal role in the detection and staging of upper tract UC. Multiphasic computed tomography urography has emerged as the imaging modality of choice, allowing comprehensive evaluation of the renal parenchyma, collecting system, ureter, and surrounding structures in a single examination. Typical imaging features include filling defects, focal wall thickening, infiltrative growth patterns with preservation of renal contour, and extension along the urothelial surface. Accurate imaging assessment is essential for differentiating UC from other centrally located renal masses and for determining the extent of multicentric involvement [7].
Management of upper tract UC depends on tumor grade, stage, and extent of disease. Radical nephroureterectomy with bladder cuff excision remains the gold standard for high-risk or multifocal tumors. The presence of multicentric disease involving the renal pelvis, ureter, and vesicoureteric junction underscores the need for meticulous surgical planning and long-term surveillance, given the high risk of recurrence and subsequent bladder involvement [8]
Case Report
A 60-year-old female presented with complaints of pain in the left
loin region for the past six months. The pain was colicky in nature,
intermittent, non-radiating, and relieved with medications. There was
no history of fever, dysuria, hematuria, vomiting or weight loss. There
was no history of hypertension, diabetes mellitus, thyroid disorders,
or prior surgeries. No similar complaints were reported in the past.
On admission, the patient was hemodynamically stable with a blood pressure of 120/70 mmHg. Per-abdominal examination revealed tenderness in the left lumbar region without palpable mass. Systemic examination was otherwise unremarkable. Based on persistent flank pain and clinical findings, further evaluation with laboratory investigations and imaging was planned
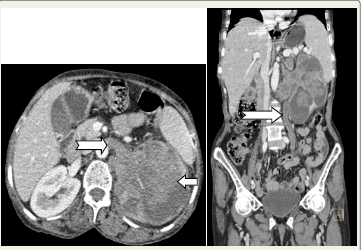
Routine blood investigations were performed and reports were available. Contrast-enhanced CT of the abdomen and pelvis revealed a large hypodense, hypoenhancing mass arising from the left renal pelvis, measuring approximately 7.4 × 7.2 cm in axial dimension and 9.8 cm in craniocaudal extent [Figure 1]. The lesion caused severe pelvicalyceal dilatation with marked thinning of renal parenchyma. Frond-like intraluminal extensions into the calyceal system were noted. Tumoral encasement of the left renal artery and extension into the left renal vein were present.
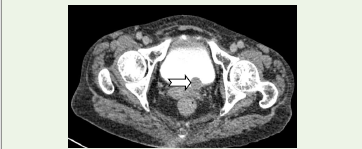
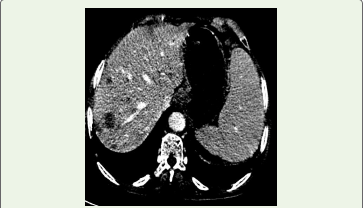
The mass showed extension into the proximal and mid left ureter with resultant dilatation, while the distal ureter appeared normal. An additional lesion was noted at the left vesicoureteric junction, producing a filling defect within the urinary bladder [Figure 2]. Enlarged left renal hilar lymph nodes were identified. Associated findings included mild hepatomegaly with multiple hypodense lesions suggestive of metastases [Figure 3] and splenomegaly.
On admission, the patient was hemodynamically stable with a blood pressure of 120/70 mmHg. Per-abdominal examination revealed tenderness in the left lumbar region without palpable mass. Systemic examination was otherwise unremarkable. Based on persistent flank pain and clinical findings, further evaluation with laboratory investigations and imaging was planned
Routine blood investigations were performed and reports were available. Contrast-enhanced CT of the abdomen and pelvis revealed a large hypodense, hypoenhancing mass arising from the left renal pelvis, measuring approximately 7.4 × 7.2 cm in axial dimension and 9.8 cm in craniocaudal extent [Figure 1]. The lesion caused severe pelvicalyceal dilatation with marked thinning of renal parenchyma. Frond-like intraluminal extensions into the calyceal system were noted. Tumoral encasement of the left renal artery and extension into the left renal vein were present.
The mass showed extension into the proximal and mid left ureter with resultant dilatation, while the distal ureter appeared normal. An additional lesion was noted at the left vesicoureteric junction, producing a filling defect within the urinary bladder [Figure 2]. Enlarged left renal hilar lymph nodes were identified. Associated findings included mild hepatomegaly with multiple hypodense lesions suggestive of metastases [Figure 3] and splenomegaly.
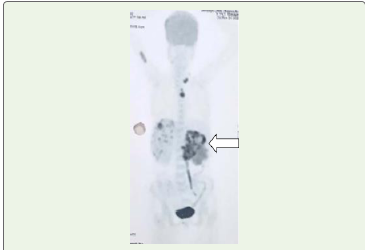
PET-CT demonstrated FDG-avid uptake within the left renal
mass, ureteric extension, renal vein involvement, and vesicoureteric
junction lesion [Figure 4], FDG uptake was also seen in few left
supraclavicular and mediastinal nodes. Intermediate uptake was seen
in the right proximal humerus, supporting a diagnosis of multicentric
urothelial malignancy with metastatic disease.
Biopsy of the renal mass was done. Histopathological examination of the specimen confirmed features consistent with UC involving the renal pelvis with associated spread. Patient was advised surgical planning after chemotherapy. Oral informed consent was obtained from the patient for publication of this case report and any accompanying images.
Biopsy of the renal mass was done. Histopathological examination of the specimen confirmed features consistent with UC involving the renal pelvis with associated spread. Patient was advised surgical planning after chemotherapy. Oral informed consent was obtained from the patient for publication of this case report and any accompanying images.
Discussion
In the present case, a 60-year-old female had an aggressive
urothelial carcinoma (UC) arising from the left renal pelvis, with
frond like intraluminal calyceal extensions, proximal and mid
ureteric extension, a distal vesicoureteric junction or bladder filling
defect, hilar nodes, renal vein involvement, and FDG avid distant
metastases (liver). This pattern is clinically coherent with UC biology,
where tumors can disseminate along the urothelial lining and present
late with obstructive and metastatic features.
A key adverse feature here is multifocal disease and ureteric
extension. Ouzzane et al. (2011) demonstrated that ureteral location
and multifocal tumors have significantly worse prognosis than
isolated renal pelvic tumors in UC treated with nephroureterectomy,
reinforcing that combined renal pelvis plus ureter involvement
represents higher risk disease [9]. Similarly, Chromecki et al. (2012)
reported that tumor multifocality is independently associated
with worse oncologic outcomes after radical nephroureterectomy,
supporting why synchronous upper tract lesions and downstream
involvement in this patient indicate aggressive behavior rather than
incidental spread [10]. The presence of a distal vesicoureteric junction
or bladder lesion is also biologically plausible through tumor seeding
and clonal evolution across the urothelium. Van Doeveren et al.
(2020) showed that bladder tumors developing after upper tract UC
are predominantly clonally derived recurrences, supporting a field
change or intraluminal seeding mechanism to explain multicentric
urothelial malignancy in a single patient [11].
Imaging findings in this case align with recognized CT urography
patterns of UC. Martingano et al. (2020) described that Upper tract
UC commonly appears as soft tissue masses, filling defects, wall
thickening, and infiltrative lesions within the collecting system,
and emphasized CT urography as the key modality for defining
local extent and differential diagnosis [12]. The described frond like
intraluminal extensions into the calyceal system are additionally
supported by histopathologic growth patterns. Sarungbam et al.
(2014) systematically evaluated Upper tract UC with intratubular
spread, highlighting that retrograde extension within renal tubular
structures is not rare and correlates with adverse clinicopathologic
features, providing a pathologic basis for the calyceal and collecting
system “frond like” appearance seen radiologically [13].
Another major prognostic marker in this patient is severe pelvicalyceal dilatation with marked cortical thinning, indicating long standing obstruction and advanced disease. Liang et al. (2016) reported that Upper tract UC accompanied by preoperative severe hydronephrosis and previous or synchronous bladder cancer has worse oncologic outcomes after radical nephroureterectomy, closely mirroring this case where severe hydronephrosis coexists with distal urothelial involvement [14]. Finally, PET CT added decisive staging value in this patient by confirming metabolically active multicentric disease, venous involvement, and distant metastases. Tanaka et al. (2014) reported that 18F FDG PET/CT can improve staging assessment in UC, particularly for metastatic disease evaluation beyond conventional imaging [15].
Another major prognostic marker in this patient is severe pelvicalyceal dilatation with marked cortical thinning, indicating long standing obstruction and advanced disease. Liang et al. (2016) reported that Upper tract UC accompanied by preoperative severe hydronephrosis and previous or synchronous bladder cancer has worse oncologic outcomes after radical nephroureterectomy, closely mirroring this case where severe hydronephrosis coexists with distal urothelial involvement [14]. Finally, PET CT added decisive staging value in this patient by confirming metabolically active multicentric disease, venous involvement, and distant metastases. Tanaka et al. (2014) reported that 18F FDG PET/CT can improve staging assessment in UC, particularly for metastatic disease evaluation beyond conventional imaging [15].
Conclusion
This case highlights the aggressive and multicentric nature of
upper tract urothelial carcinoma, demonstrating rare synchronous
involvement of the renal pelvis, ureter, and vesicoureteric junction
with vascular invasion and distant metastases. The findings emphasize
the concept of pan-urothelial susceptibility and intraluminal tumor
spread, accounting for multifocal disease and advanced presentation.
Comprehensive imaging, particularly CT urography and FDG PETCT,
was pivotal in accurately delineating disease extent and staging.
Early recognition of such extensive involvement is essential, as
multicentric UC is associated with poorer prognosis and mandates
radical surgical management combined with vigilant oncologic
follow-up and surveillance.
References
Citation
Tapashetti S, Rani RV, Chandrahas A, Sandhya R. Multicentric Urothelial Cell Carcinoma Involving Renal Pelvis, Ureter, and Vesicoureteric Junction: A Case Report. Indian J Appl Radiol. 2026;12(1): 228.