Case Report
Adenoma Malignum in Peutz Jegher Syndrome: Case Report
Riya Fathima1, Thara Pratap1, Pushpa Mahadevan2, Rashmi Unnikrishnan2, Dhanya Jacob1 and Muhammed Jasim Abdul Jalal3*
1Radiology, VPS Lakeshore Hospital, Kochi, India,
2Pathology, VPS Lakeshore Hospital, Kochi, India,
3Internal Medicine and Rheumatology, Olive Health Care, Thrissur, India
2Pathology, VPS Lakeshore Hospital, Kochi, India,
3Internal Medicine and Rheumatology, Olive Health Care, Thrissur, India
*Corresponding author:Muhammed Jasim Abdul Jalal, Department of Internal Medicine and Rheumatology, Olive Healthcare, Thrissur, Kerala, India Email: jasimabduljalal@yahoo.com
Copyright: ©2026 Fathima R, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article Information:Submission: 18/12/2025; Accepted: 24/03/2026; Published: 28/03/2026
Abstract
Adenoma malignum, also known as gastric-type mucinous adenocarcinoma of the cervix, is a rare variant of mucinous adenocarcinoma, previously referred to as minimal deviation adenocarcinoma. It accounts for approximately 1–3% of all cervical adenocarcinomas. Adenoma malignum is often associated
with Peutz-Jeghers syndrome and mucinous tumors of the ovary. This case is unique due to its prolonged indolent clinical course, with no evidence of local invasion or metastasis over a period of six years, underscoring the deceptively benign clinical, radiological, and pathological appearance of this malignancy.
We emphasize the subtle diagnostic clues that can facilitate early recognition of this rare but aggressive entity.
Keywords:Adenoma malignum; Cervical cancer; Peutz–Jeghers syndrome
Introduction
Adenoma malignum of the cervix is a rare subtype of cervical
adenocarcinoma. This tumor is characterized by its deceptively
benign appearance on imaging and histopathology, often resulting
in delayed diagnosis. Adenoma malignum may arise de novo or in
association with Peutz–Jeghers syndrome or hereditary intestinal
polyposis. We report a case of adenoma malignum in a patient with
known Peutz–Jeghers syndrome, with a six-year interval between the
initial presentation and definitive diagnosis.
Case Report
A 45-year-old nulliparous woman, diagnosed with Peutz–Jeghers
syndrome (PJS) during adolescence based on perioral pigmentation
and multiple gastrointestinal polyps, presented with mild mucinous
vaginal discharge. Her past medical history was significant for
multiple admissions due to small bowel obstruction and surgical
interventions for polyp-associated intussusception.
On per-vaginal examination, the cervix appeared bulky with
mucoid discharge. Transvaginal ultrasound revealed a multiloculated
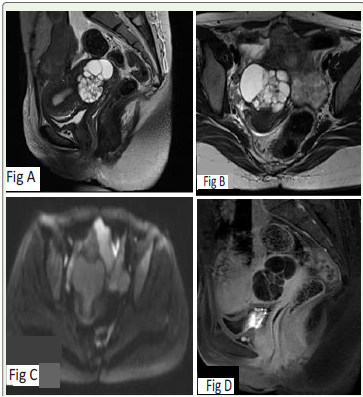
cystic lesion within the cervix. Pelvic MRI was subsequently
performed, showing an enlarged cervix with a multiloculated cystic
lesion that was T2 hyperintense and T1 hypointense, extending
into the deep stroma. Post-contrast imaging demonstrated thick
enhancing septa [Figure 1].
Given the patient’s background of PJS, a differential diagnosis
of adenoma malignum was suggested, despite the absence of a solid
component. The patient, however, declined surgical intervention and
opted for regular follow-up. The lesion remained stable for nearly
three years, after which she was lost to follow-up.
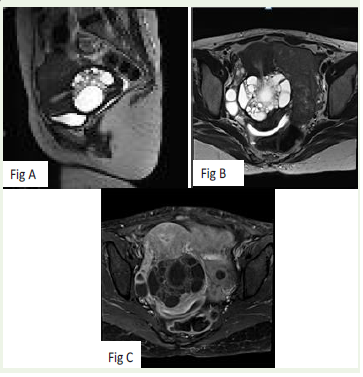
Three years later, she re-presented with profuse mucinous vaginal
discharge. Local examination again revealed a bulky cervix, and repeat
MRI was performed for reassessment [Figure 2]. Compared with the
initial MRI, there was mild further enlargement of the lesion with
stromal expansion. Post-contrast imaging showed a minimal increase
in wall thickness, but no definite solid component was identified.
There was no evidence of parametrial extension, pelvic, or inguinal
lymphadenopathy. In view of the progressive nature of the lesion and
persistent symptoms, adenoma malignum was strongly suspected,
and the patient consented to surgery.
Unlike conventional cervical malignancies, adenoma malignum predominantly involves the deep cervical stroma while sparing the mucosa; therefore, surface biopsy may be non-diagnostic and was not attempted.
Unlike conventional cervical malignancies, adenoma malignum predominantly involves the deep cervical stroma while sparing the mucosa; therefore, surface biopsy may be non-diagnostic and was not attempted.
She subsequently underwent total abdominal hysterectomy.
Gross examination revealed an enlarged cervix with a
multiloculated cystic neoplasm measuring 5.6 × 4.5 × 4.5 cm. The
cysts ranged in size from 0.3 to 2 cm and contained viscous fluid.
The inner walls of the cysts were smooth, with no solid or papillary
areas identified. Microscopy showed well-formed glands and cysts
of variable sizes haphazardly distributed within the stroma, with
minimal desmoplastic response. The tumor cells exhibited minimal
cytologic atypia and abundant pale eosinophilic to clear cytoplasm
with distinct cell borders. The tumor involved the deep third of the
cervical stroma but spared the resection margins (clearance of 0.1
cm). The histopathological features were consistent with gastric-type
adenocarcinoma circumferentially involving the cervix, confirming
the diagnosis of adenoma malignum. The tumor was staged as FIGO
IB2, TNM T1b2N0.
As the surgical margins were negative, the multidisciplinary tumor board recommended follow-up. PET-CT excluded distant metastases and other malignancies associated with PJS. At present, the patient is two years post-surgery and remains disease-free, with no evidence of metastasis.
As the surgical margins were negative, the multidisciplinary tumor board recommended follow-up. PET-CT excluded distant metastases and other malignancies associated with PJS. At present, the patient is two years post-surgery and remains disease-free, with no evidence of metastasis.
Discussion
Adenoma malignum, also known as gastric-type mucinous
adenocarcinoma of the cervix, is a rare variant of mucinous
adenocarcinoma, previously termed minimal deviation
adenocarcinoma. It accounts for 1–3% of all cervical adenocarcinomas
and is often associated with Peutz–Jeghers syndrome and mucinous
ovarian tumors [1].
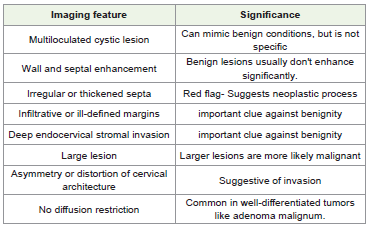
Classically, adenoma malignum has been described as a multilocular cystic lesion with enhancing solid components, cervical enlargement, and deep stromal invasion. In our case, cervical expansion and deep stromal invasion were present; however, solid components were not appreciable, even on retrospective review. The initial MRI revealed a multiloculated cystic cervical lesion with enhancing septa and walls, but without a solid component—features that overlap with benign lesions such as complex nabothian cysts, tunnel clusters, or deep endocervical glandular hyperplasia [2]. Nonetheless, the involvement of deep stroma, along with intense enhancement of septa and a gradual increase in septal thickness and cyst size on follow-up MRI, raised concern and ultimately led to surgical excision and a definitive diagnosis of adenoma malignum. Differentiating benign entities from adenoma malignum is particularly challenging when an enhancing solid component is absent. Several reports have documented benign glandular lesions— including tunnel clusters, deep endocervical glands, deep nabothian cysts, and lobular endocervical glandular hyperplasia—that can closely mimic adenoma malignum both histologically and radiologically [3]. Benign lesions generally do not invade the deep cervical stroma, are smaller in size, demonstrate well-defined margins, and typically lack solid components. The transition from hyperplasia to highgrade malignancy appears to represent a continuous spectrum, with the proportion of solid components within a lesion serving as a key determinant. Profuse mucinous vaginal discharge is the most common clinical presentation. The risk is heightened in patients with Peutz– Jeghers syndrome, who have a significantly increased lifetime risk of gynecologic malignancies, particularly adenoma malignum. Therefore, close surveillance is warranted in such high-risk populations. MRI plays a pivotal role in early detection. Adenoma malignum often appears as a multicystic lesion with a characteristic “honeycomb” appearance, thin septations, and variable wall or septal enhancement [Table 1]. While the presence of a solid component or nodularity raises suspicion for malignancy, cases such as ours-entirely cystic without a solid nodule—pose diagnostic difficulty. On MRI, these lesions are usually isointense or slightly hyperintense relative to the uterus on T1-weighted imaging and markedly hyperintense on T2-weighted imaging. A T2 hyperintense solid component, when present adjacent to cysts, may enhance following gadolinium administration. Radiologic–pathologic correlation has shown that these apparent solid areas often represent clusters of minute cysts with edematous cervical stroma rather than true solid tissue [4]. Thus, the absence of a solid component on imaging does not exclude malignancy, as microcysts or stromal edema may mimic cystic spaces. However, true solid nests may be observed in aggressive or dedifferentiated forms.
Classically, adenoma malignum has been described as a multilocular cystic lesion with enhancing solid components, cervical enlargement, and deep stromal invasion. In our case, cervical expansion and deep stromal invasion were present; however, solid components were not appreciable, even on retrospective review. The initial MRI revealed a multiloculated cystic cervical lesion with enhancing septa and walls, but without a solid component—features that overlap with benign lesions such as complex nabothian cysts, tunnel clusters, or deep endocervical glandular hyperplasia [2]. Nonetheless, the involvement of deep stroma, along with intense enhancement of septa and a gradual increase in septal thickness and cyst size on follow-up MRI, raised concern and ultimately led to surgical excision and a definitive diagnosis of adenoma malignum. Differentiating benign entities from adenoma malignum is particularly challenging when an enhancing solid component is absent. Several reports have documented benign glandular lesions— including tunnel clusters, deep endocervical glands, deep nabothian cysts, and lobular endocervical glandular hyperplasia—that can closely mimic adenoma malignum both histologically and radiologically [3]. Benign lesions generally do not invade the deep cervical stroma, are smaller in size, demonstrate well-defined margins, and typically lack solid components. The transition from hyperplasia to highgrade malignancy appears to represent a continuous spectrum, with the proportion of solid components within a lesion serving as a key determinant. Profuse mucinous vaginal discharge is the most common clinical presentation. The risk is heightened in patients with Peutz– Jeghers syndrome, who have a significantly increased lifetime risk of gynecologic malignancies, particularly adenoma malignum. Therefore, close surveillance is warranted in such high-risk populations. MRI plays a pivotal role in early detection. Adenoma malignum often appears as a multicystic lesion with a characteristic “honeycomb” appearance, thin septations, and variable wall or septal enhancement [Table 1]. While the presence of a solid component or nodularity raises suspicion for malignancy, cases such as ours-entirely cystic without a solid nodule—pose diagnostic difficulty. On MRI, these lesions are usually isointense or slightly hyperintense relative to the uterus on T1-weighted imaging and markedly hyperintense on T2-weighted imaging. A T2 hyperintense solid component, when present adjacent to cysts, may enhance following gadolinium administration. Radiologic–pathologic correlation has shown that these apparent solid areas often represent clusters of minute cysts with edematous cervical stroma rather than true solid tissue [4]. Thus, the absence of a solid component on imaging does not exclude malignancy, as microcysts or stromal edema may mimic cystic spaces. However, true solid nests may be observed in aggressive or dedifferentiated forms.
In a study by Sugiyama et al., the MR findings of pseudoneoplastic
glandular lesions were reported to be almost identical to those of
adenoma malignum, making differentiation extremely challenging
[5].
Histologically, adenoma malignum is so well-differentiated both structurally and cytologically that a diagnosis of malignancy can only be established based on the presence of distorted, irregularly outlined glands deep within the cervix or atypical cells. Its deceptively benign appearance often leads to diagnostic difficulty.
Routine cytological screening is of limited value in adenoma malignum. Therefore, a deep biopsy is essential when clinical suspicion is high, especially in patients presenting with profuse vaginal discharge and a multilocular cystic cervical mass [6]. Some studies suggest that the prognosis of adenoma malignum is better than that of conventional cervical adenocarcinoma [6]. Reports indicate that up to 60% of adenoma malignum cases with a solid component present with metastases [3]. However, our case demonstrated an indolent course, with no evidence of metastasis even after six years from initial presentation and two years postoperatively.
The mainstay of treatment for adenoma malignum is surgical excision. However, no standardized surgical protocol has been established due to its rarity, frequent preoperative misdiagnosis, and limited data on surgical outcomes [7]. Due to the rarity of the disease, standardized surveillance and follow-up guidelines are not well established. Common sites of recurrence include local pelvic recurrence, pelvic lymph nodes, and para-aortic lymph nodes. MRI is the preferred modality for detecting local recurrence, while CT imaging is recommended for evaluating distant metastasis.
Histologically, adenoma malignum is so well-differentiated both structurally and cytologically that a diagnosis of malignancy can only be established based on the presence of distorted, irregularly outlined glands deep within the cervix or atypical cells. Its deceptively benign appearance often leads to diagnostic difficulty.
Routine cytological screening is of limited value in adenoma malignum. Therefore, a deep biopsy is essential when clinical suspicion is high, especially in patients presenting with profuse vaginal discharge and a multilocular cystic cervical mass [6]. Some studies suggest that the prognosis of adenoma malignum is better than that of conventional cervical adenocarcinoma [6]. Reports indicate that up to 60% of adenoma malignum cases with a solid component present with metastases [3]. However, our case demonstrated an indolent course, with no evidence of metastasis even after six years from initial presentation and two years postoperatively.
The mainstay of treatment for adenoma malignum is surgical excision. However, no standardized surgical protocol has been established due to its rarity, frequent preoperative misdiagnosis, and limited data on surgical outcomes [7]. Due to the rarity of the disease, standardized surveillance and follow-up guidelines are not well established. Common sites of recurrence include local pelvic recurrence, pelvic lymph nodes, and para-aortic lymph nodes. MRI is the preferred modality for detecting local recurrence, while CT imaging is recommended for evaluating distant metastasis.
Conclusion
Adenoma malignum is a rare entity with significant diagnostic
challenges, primarily due to its overlap with benign imaging
appearances. The key imaging feature is a multiloculated cystic
lesion of the cervix with deep stromal invasion. An enhancing solid
component may also be present. A high index of clinical suspicion,
particularly in genetically predisposed patients, along with the
presence of mucous vaginal discharge is crucial for diagnosis. Early
surgical intervention may be warranted to prevent diagnostic delays
and improve prognosis.
Conflict of Interest:The authors have no conflict of interest.
Declaration of the patient consent form: Patient consent form attached.
Declaration of the patient consent form: Patient consent form attached.
References
Citation
Fathima R, Pratap T, Mahadevan P, Unnikrishnan R, Jacob D, et al. Adenoma Malignum in Peutz Jegher Syndrome: Case Report. Indian J Appl Radiol. 2026;12(1): 227.