Research Article
Balancing Clinical Judgment and Imaging: Evaluation of Pulmonary Embolism Using Modified Wells Score, Age-Adjusted D-Dimer, and CT Pulmonary Angiography
Indushree TV*, Shyam S, Akshay H Janakare and Parthasarathy KR
Department of Radiodiagnosis, SS Institute of Medical Sciences and Research Centre, Davangere, Karnataka, India
*Corresponding author:Dr. Indushree TV, Department of Radiodiagnosis, SS Institute of Medical Sciences and Research Centre, Davangere, Karnataka, India. E-mail Id: indushreetv@gmail.com
Copyright: © 2026 Indushree TV, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article Information:Submission: 12/02/2026; Accepted: 23/03/2026; Published: 26/03/2026
Abstract
Objective: To evaluate the diagnostic performance of the Modified Wells Score and age-adjusted D-dimer values in predicting pulmonary embolism and to correlate these findings with computed tomography pulmonary angiography (CTPA).
Materials and Methods: This prospective analytical study included 77 patients clinically suspected of pulmonary embolism who were referred for computed tomography pulmonary angiography. Modified Wells Score categorization, standard and age-adjusted D-dimer values were recorded and correlated with CTPA findings.
Results: Pulmonary embolism was detected on CTPA in both Wells-likely and Wells-unlikely groups. Age-adjusted D-dimer demonstrated improved negative predictive value in the pulmonary embolism unlikely group, reducing unnecessary CTPA examinations.
Conclusion: An integrated diagnostic approach combining Modified Wells Score, age-adjusted D-dimer, and CTPA improves diagnostic accuracy and optimizes utilization of imaging in suspected pulmonary embolism.
Materials and Methods: This prospective analytical study included 77 patients clinically suspected of pulmonary embolism who were referred for computed tomography pulmonary angiography. Modified Wells Score categorization, standard and age-adjusted D-dimer values were recorded and correlated with CTPA findings.
Results: Pulmonary embolism was detected on CTPA in both Wells-likely and Wells-unlikely groups. Age-adjusted D-dimer demonstrated improved negative predictive value in the pulmonary embolism unlikely group, reducing unnecessary CTPA examinations.
Conclusion: An integrated diagnostic approach combining Modified Wells Score, age-adjusted D-dimer, and CTPA improves diagnostic accuracy and optimizes utilization of imaging in suspected pulmonary embolism.
Keywords:Pulmonary embolism; Modified Wells score; Age-adjusted D-dimer; CT pulmonary angiography
Introduction
Pulmonary embolism (PE) is the third most common acute
cardiovascular condition after myocardial infarction and stroke and
represents a major cause of morbidity and mortality worldwide. Early
diagnosis and prompt initiation of treatment are essential because
untreated PE carries a high mortality rate, whereas appropriate
anticoagulation therapy significantly reduces morbidity and mortality.
The clinical presentation of PE is often nonspecific, including symptoms
such as dyspnea, chest pain, tachycardia, and syncope. Because these
features overlap with several cardiopulmonary disorders, diagnosis
based solely on clinical findings can be challenging. Therefore, clinical
prediction rules have been developed to estimate the probability of PE
and guide further diagnostic testing. The Modified Wells Score is one
of the most commonly used clinical prediction tools for stratifying
patients into low or high probability categories. Patients classified as
low probability can undergo D-dimer testing to exclude PE without
imaging. However, the specificity of conventional D-dimer testing
decreases with increasing age because several clinical conditions can
elevate D-dimer levels. To overcome this limitation, age-adjusted
D-dimer thresholds have been proposed. This strategy increases the
D-dimer cut-off value according to patient age, thereby improving
specificity and reducing unnecessary imaging studies in elderly
patients. Computed tomography pulmonary angiography (CTPA) has
emerged as the reference standard imaging modality for diagnosing
pulmonary embolism due to its high sensitivity and specificity and its
ability to identify alternative thoracic pathologies. The present study
aimed to evaluate the diagnostic performance of the Modified Wells
Score and age-adjusted D-dimer values in predicting pulmonary
embolism and to correlate these findings with CT pulmonary
angiography, thereby assessing the effectiveness of a combined
diagnostic approach. [1-5].
Review of literature
Although several studies have evaluated the role of the Modified
Wells score and D-dimer testing in the diagnosis of pulmonary
embolism, important limitations remain. Previous research has
demonstrated that combining clinical prediction rules with D-dimer
testing can improve diagnostic sensitivity and help exclude pulmonary
embolism; however, the specificity of conventional D-dimer testing
is low, particularly in elderly patients, leading to a high rate of falsepositive
results and unnecessary imaging investigations. Recent studies
have suggested that age-adjusted D-dimer thresholds may improve
diagnostic efficiency by increasing specificity without compromising
safety. Nevertheless, there is limited data evaluating the combined
diagnostic performance of Modified Wells score and age-adjusted
D-dimer values with correlation to CT pulmonary angiography,
particularly in tertiary care hospital settings. Therefore, the present
study aims to assess the diagnostic utility of these parameters and
their correlation with CT pulmonary angiography in patients with
suspected pulmonary embolism.
Materials And Methods
Ethics Statement: The study was approved by the Institutional
Ethics Committee, and informed consent was obtained from all
participants.
Study Design: Prospective analytical study.
Study Setting: The study was conducted in the Department of Radiodiagnosis at S.S. Institute of Medical Sciences and Research Centre over a period of two years.
Study Population: A total of 77 patients clinically suspected of pulmonary embolism who were referred for CT pulmonary angiography were included.
Study Design: Prospective analytical study.
Study Setting: The study was conducted in the Department of Radiodiagnosis at S.S. Institute of Medical Sciences and Research Centre over a period of two years.
Study Population: A total of 77 patients clinically suspected of pulmonary embolism who were referred for CT pulmonary angiography were included.
Inclusion Criteria:
Patients referred for CT pulmonary angiography from outpatient
or inpatient departments.Patients with clinical suspicion of pulmonary embolism.
Exclusion Criteria:
Follow-up cases of pulmonary embolismPatients with contrast allergy
Patients with renal failure
Patients on anticoagulation therapy
Patients unwilling to provide consent
Clinical Assessment
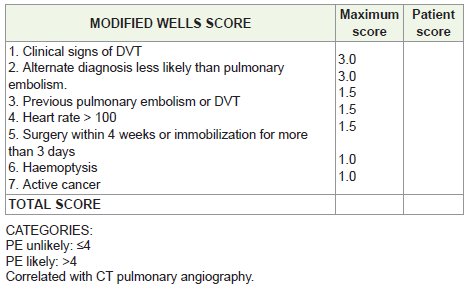
The Modified Wells Score was calculated for each patient and categorized as:
PE unlikely: ≤4
PE likely: >4
Laboratory Assessment
D-dimer levels were measured using immunofluorescence technology.
Standard cut-off: 500 ng/mL
Age-adjusted cut-off: Age × 10 ng/mL for patients >50 years
CT Pulmonary Angiography Protocol::
CT pulmonary angiography was performed using a multidetector CT scanner
according to the standard institutional protocol with intravenous
administration of iodinated contrast. 80–100 ml of non-ionic
iodinated contrast was injected at 4–5 ml/s using a power injector,
followed by a saline flush. Images were reconstructed in axial, coronal,
and sagittal planes to evaluate the pulmonary arterial tree. CTPA
images were independently reviewed by two experienced radiologists
blinded to the clinical probability scores and D-dimer results.Statistical Analysis:
Statistical analysis was performed using appropriate statistical
software. Quantitative data were expressed as mean ± standard
deviation, while categorical variables were expressed as frequencies
and percentages. Diagnostic performance parameters including
sensitivity, specificity, PPV, NPV, and ROC analysis were calculated.
A p-value <0.05 was considered statistically significant.Results
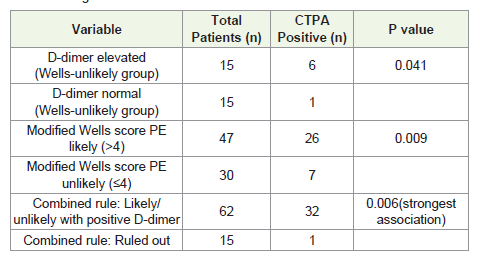
Out of 77 patients evaluated, Pulmonary embolism was detected
on CTPA in both the Modified Wells score “likely” and “unlikely”
categories. A subset of patients categorized as pulmonary embolism
unlikely demonstrated positive findings on CTPA, highlighting the
limitations of clinical scoring alone. D-dimer values were interpreted
using age-adjusted thresholds before correlation with CTPA findings.
Age-adjusted D-dimer values demonstrated higher negative predictive
value in the pulmonary embolism unlikely group when compared to
standard cutoff values, reducing unnecessary CTPA examinations.
False-positive and false-negative results were observed, emphasizing
the importance of an integrated diagnostic approach [4-5].
Demographic Characteristics:
The study included 77 patients, with a mean age of 49.05 ± 18.68
years. The majority of patients were between 31 and 70 years of age.
Males constituted 58.4% of the study population.Clinical Characteristics:
Clinical signs of deep vein thrombosis were present in 11.7% of
patients. Recent surgery or prolonged immobilization was observed in
40.3%, while tachycardia (>100 bpm) was noted in 42.9% of patients.Wells Score Distribution:
Based on the Modified Wells Score:
• PE likely: 47 patients (61%)
• PE unlikely: 30 patients (39%)
D-Dimer Levels
Elevated D-dimer levels (>500 ng/mL) were observed in 76.6% of patients.
CTPA Findings:
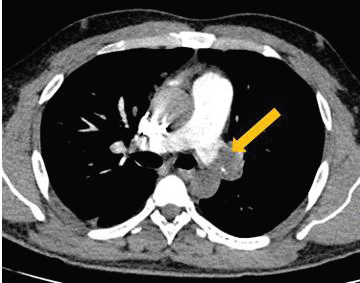
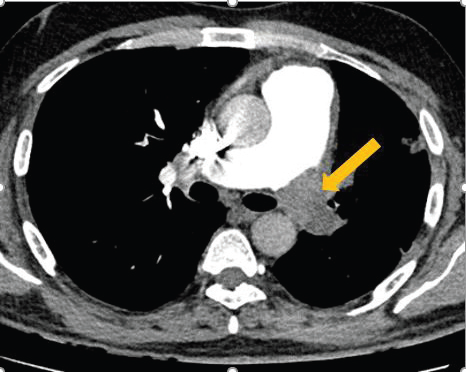
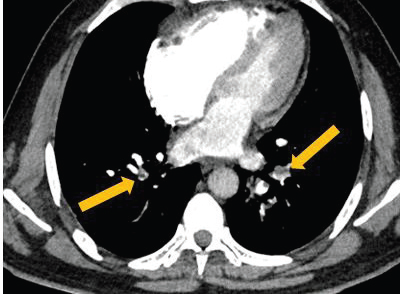
CT pulmonary angiography confirmed pulmonary embolism in
33 patients (42.9%), while 44 patients (57.1%) showed no evidence
of embolism.The most common site of embolism was the main pulmonary artery (20.8%), followed by segmental arteries (15.6%) and subsegmental arteries (15.6%).
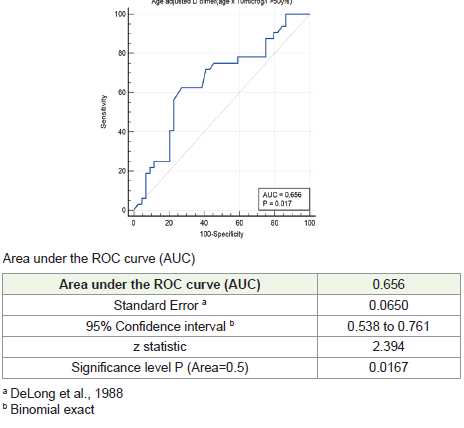
Diagnostic Performance:
Standard D-dimer testing demonstrated high sensitivity but low
specificity, whereas age-adjusted D-dimer improved specificity.
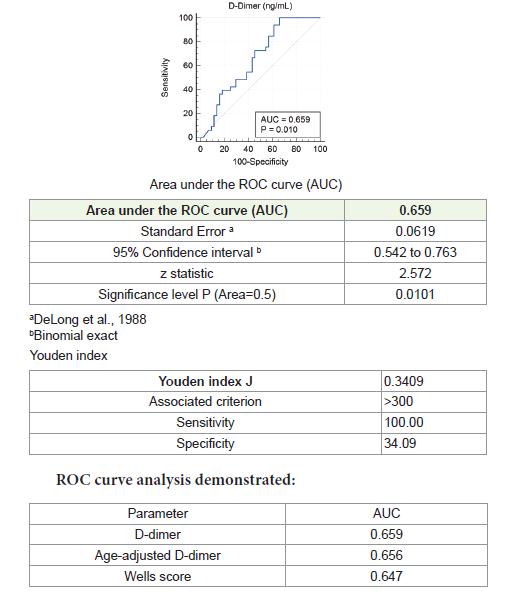
The ROC analysis showed an area under the curve (AUC) of 0.659,
indicating modest diagnostic performance of D-dimer in predicting
PE. The result was statistically significant (p = 0.0101).
Standard D-dimer testing demonstrated high sensitivity but low
specificity, whereas age-adjusted D-dimer improved specificity.
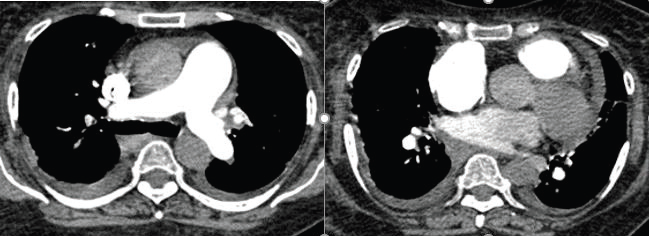
Alternative Diagnoses::
CTPA also identified alternative diagnoses including:
• Pleural effusion• Pulmonary edema
• Pneumonia
• Emphysema
• Malignancy
Discussion
The diagnosis of pulmonary embolism remains challenging due
to its nonspecific clinical presentation and potentially fatal outcome.
Clinical prediction rules combined with laboratory testing and
imaging have therefore become essential components of diagnostic
algorithms.
The Modified Wells Score demonstrated moderate diagnostic accuracy in this study, consistent with previous studies. While it is useful for risk stratification, clinical scoring alone cannot reliably exclude pulmonary embolism. D-dimer testing has high sensitivity but limited specificity. Age-adjusted D-dimer thresholds have been proposed to improve specificity, particularly in elderly patients. Our findings support the use of age-adjusted thresholds to reduce unnecessary imaging. CT pulmonary angiography remains the definitive imaging modality for diagnosing PE, providing direct visualization of intraluminal filling defects and allowing identification of alternative thoracic pathologies. The results of this study support the use of a combined diagnostic strategy incorporating clinical scoring, laboratory testing, and imaging [4,5] [7,8] [9,12].
The Modified Wells Score demonstrated moderate diagnostic accuracy in this study, consistent with previous studies. While it is useful for risk stratification, clinical scoring alone cannot reliably exclude pulmonary embolism. D-dimer testing has high sensitivity but limited specificity. Age-adjusted D-dimer thresholds have been proposed to improve specificity, particularly in elderly patients. Our findings support the use of age-adjusted thresholds to reduce unnecessary imaging. CT pulmonary angiography remains the definitive imaging modality for diagnosing PE, providing direct visualization of intraluminal filling defects and allowing identification of alternative thoracic pathologies. The results of this study support the use of a combined diagnostic strategy incorporating clinical scoring, laboratory testing, and imaging [4,5] [7,8] [9,12].
Conclusion
A combined diagnostic approach using Modified Wells Score, age adjusted
D-dimer testing, and CT pulmonary angiography improves
diagnostic accuracy in patients with suspected pulmonary embolism.
Age-adjusted D-dimer thresholds help reduce unnecessary imaging,
particularly in elderly patients, while maintaining diagnostic safety.
[4,5].
Limitations:
1. Single-center study2. Small sample size
3. Lack of long-term follow-up
Further multicenter studies are required to validate these findings.
Conflict of Interest Statement:
The authors declare no conflict of interest.References
Citation
Indushree TV, Shyam S, Akshay H Janakare, Parthasarathy KR. Balancing Clinical Judgment and Imaging: Evaluation of Pulmonary Embolism Using Modified Wells Score, Age-Adjusted D-Dimer, and CT Pulmonary Angiography. Indian J Appl Radiol. 2026;12(1): 226.