Case Report
Spontaneous Aorto-Pulmonary Artery Fistula Secondary to Ruptured Aortic Arch Aneurysm Presenting as Acute High Output Cardiac Failure
Sayed S*, Katiyar G, Mulla M, Kumar P and Desai M
Department of Radiodiagnosis and Interventional Radiology Goa Medical College and Hospitals, Goa, India
*Corresponding author:Shoaib Sayed, Department of Radiodiagnosis and Interventional Radiology Goa Medical College and Hospitals, Goa, India. E-mail Id: shoaibsayed2699@yahoo.com
Copyright: © 2025 Sayed S, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article Information:Submission: 22/09/2024; Accepted: 10/02/2025; Published: 15/02/2025
Abstract
Aorto-pulmonary artery fistula is an uncommon consequence of chronic thoracic aortic aneurysm and is mostly caused by pressure erosion. This can be aggravated by infection, trauma, surgery and is rarely spontaneous. Cross-sectional imaging in patients with unexplained acute onset high output cardiac failure is a warranted investigation to diagnose fistulous communication between great vessels i.e. aorta and pulmonary arteries, outline the anatomy, diagnose secondary complications and in effectively guiding the management.
Introduction
Aorto-pulmonary fistulas are rare complications of usually
thoracic aortic aneurysms and can present with sudden onset high
output failure. The modality of treatment is usually surgical with
endovascular treatments coming up in the recent past. It is an
emergency and has high mortality rates if left untreated.
Case Presentation
A 55-year-old male, a known hypertensive on medication,
was brought to the emergency department with sudden onset of
breathlessness, sweating and dry cough. The breathlessness had
worsened to grade IV NYHA over a period of 4 days. There were no
complaints of chest pain, palpitations and swelling of lower limbs.
Examination revealed pulse rate of 90 beats/minute and blood pressure
of 110/70mmHg. Hoarseness of voice was noted with engorged neck
veins. Fine crepitations were heard in the right infra-scapular region.
Continuous murmur was noted on auscultation in the aortic area.
Left vocal cord palsy was noted on indirect laryngoscopy which was
performed to evaluate hoarseness of voice.
ECG showed T-wave inversion in the lead I and avL, reflecting left atrial enlargement.
ECG showed T-wave inversion in the lead I and avL, reflecting left atrial enlargement.
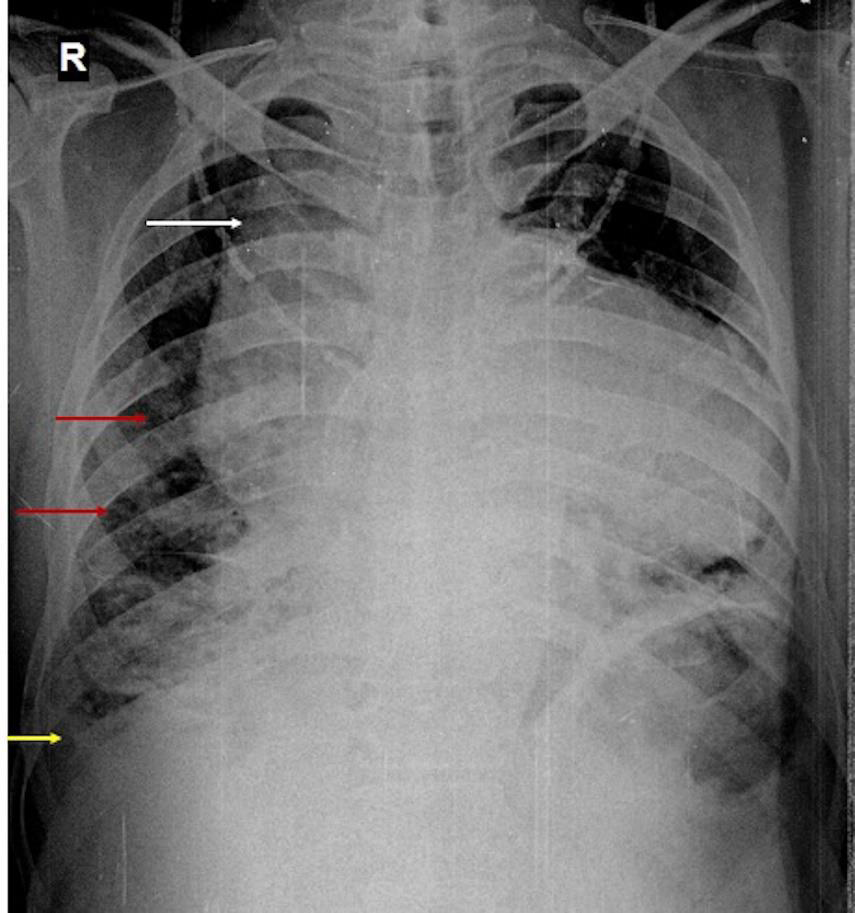
Chest X-ray [Figure 1] performed revealed mediastinal widening,
cardiomegaly with right chamber enlargement with an upturned
cardiac apex. The right hilar and perihilar vascular markings were
prominent with ipsilateral peribronchial cuffing. There was blunting
of right costophrenic angle suggestive of pleural effusion. These
features with clinical correlation represented congestive cardiac
failure with unilateral cardiogenic pulmonary oedema.
Laboratory investigations revealed Hb of 13.6mg%, total
leucocyte count 5700mg/ml, platelet count of 1.3 lakhs, urea 34mg/
dl, creatinine 1.0 mg/dl, troponin I 0.085ng/ml (normal upto 0.04ng/
ml), serum CK-MB 1.3ng/ml (normal upto 5ng/ml) and positive Ddimer
test.
2D echocardiography revealed dilated right atrium and right
ventricle with severe pulmonary arterial hypertension (PASP
80mmHg) and moderate tricuspid regurgitation. IVC was dilated and
non collapsing. LVEF 60%. No regional wall motion abnormalities
were seen. No pericardial effusion was present. However, orthopnoea
limited detailed evaluation.
In view of the elevated D-dimer and the chest X-ray and
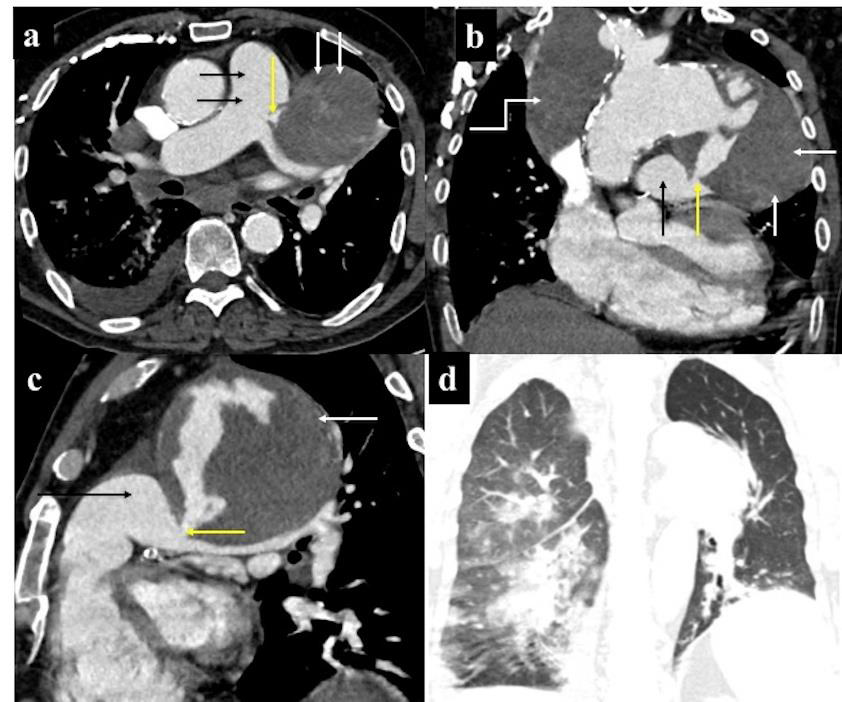
echocardiographic findings, CT pulmonary angiography [Figure 2a-d] was performed to rule out pulmonary thromboembolism.
CT showed ectatic ascending aorta, measuring 4.7cm in diameter
with intimal calcification involving ascending aorta and aortic arch.
Large saccular aneurysm was seen arising from the inferior wall of
the distal aortic arch (9.8 x 9.6 x 9.2 cm) with a wide neck of 6.8
cm and a peripheral intraluminal thrombus. Communication was
seen between the aortic aneurysm and main pulmonary artery over
a length of 8 mm representing aorto-pulmonary artery fistula. The
aortic aneurysm was compressing the left pulmonary artery with
dilatation of the main and right pulmonary artery. No evidence of
pulmonary thrombo-embolism was seen. Cardiomegaly was noted
with dilated right atrium, right ventricle and dilated IVC. Moderate
right sided pleural effusion was seen. On the lung reformatted
images, patchy alveolar air space disease was present in the right lung,
suggestive of right-sided pulmonary edema. Left lung parenchyma
was normal. Another partly-thrombosed saccular aneurysm of the
right innominate artery (9 x 6.8 x 6 cm) was seen compressing the
superior vena cava with multiple venous collaterals along the right
anterolateral chest wall.
Digital subtraction angiography [Figure 3a,b] performed
subsequently, confirmed the aortic aneurysm and aorto-pulmonary
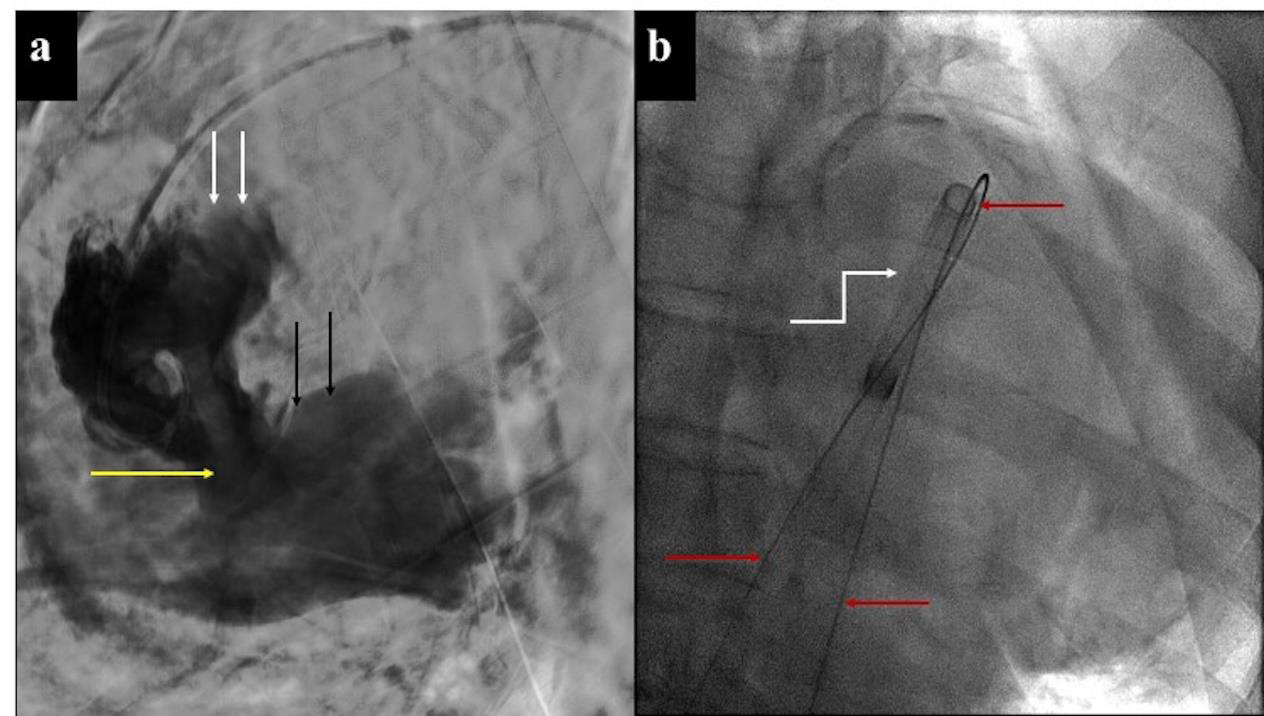
artery fistula and delineated the precise location and size of the
fistulous communication (22mm) using multiple projections. Ostial
stenosis was noted of LCA. Surgical option was given but declined by
the relative in view of high risk. Urgent interventional percutaneous
placement of closure device was thus planned. Pigtail catheter was
placed in the ascending aorta and contrast injection demonstrated
the fistula. The fistulous communication was engaged from the
aortic aspect. The terumo guide wire was introduced and advanced
to form aorto-venous loop by snaring from the venous access
through main pulmonary artery. The placement sheath of Flex II
ASD occlusive device (33mm waist) was placed over the guide wire.
However unfortunately during the intervention sudden clinical and
hemodynamic deterioration resulted in cardiac arrest and the patient
succumbed, despite all attempts to revive him.
Discussion
Aneurysms of the thoracic aorta may present with chest pain,
thrombo-embolism resulting in stroke, compressive symptoms
like recurrent laryngeal nerve compression resulting in hoarseness
of voice, dysphagia due to esophageal compression etc. or may be
asymptomatic [1]. They can be complicated by aortic dissection,
rupture, congestive heart failure, and fistulous communication with
adjoining structures including aorto-pulmonary, aorto-bronchial
and aorto-esophageal fistula.
Aorto-pulmonary arterial fistula occurs when the wall of a
degenerative or false aortic aneurysm rupture into the pulmonary
arterial circulation due to pressure erosion caused by pulsatile friction
[2,3]. Most of the fistulae originate from the ascending aorta; fistulous
communication between the distal aortic arch or the descending
aorta to the pulmonary artery is quite rare [4]. It can be seen in posttraumatic
or post-operative setting and in infective conditions like
pneumonia, lung abscess. The fistula causes volume overload in the
pulmonary arterial circulation and is fatal if not treated timely [5].
The presentation is acute with chest pain, hemoptysis, orthopnea and
paroxysmal nocturnal dyspnea
In our case, there was neither previous history of surgery nor
hemoptysis. Since there was no significant past history, the duration
of the aortic aneurysm being asymptomatic remains unclear.
The left to right shunt caused by the fistulous communication
between the major vessels caused a high output failure, resulting
in pulmonary edema, pleural effusion and moderate pulmonary
hypertension.
Chest X-ray shows mediastinal widening, which is contributed
by the aortic aneurysm and/ or SVC dilatation. Pulmonary artery
segment appears prominent and dilated in pulmonary arterial
hypertension. Perihilar patchy opacities in characteristic “batwing”
pattern with Kerley A and B lines may be present along with
cephalisation, suggestive of pulmonary edema. “Meniscus’’ sign may
be present with blunting of costophrenic angle signifying pleural
effusion. Cardiomegaly with outward shift of the apex of the heart, if
present, represents right ventricular dilatation in right heart failure.
2D echocardiography helps in visualising the cardiac anatomy
i.e. cardiac chambers for size, valves, pericardial cavity, inferior and
superior vena cava as well as physiology i.e. wall motion abnormality,
valvular dysfunction and ejection fraction. Doppler-mode shows
continuous flow in the pulmonary artery and increased pulmonary
arterial pressure in aorto-pulmonary arterial fistula. The fistulous
communication may also be visualised.
CT angiography is non-invasive modality for evaluation of
unexplained high output cardiac failure owing to high spatial
resolution, for the presence of aneurysm, fistulous communication
of the aneurysm with adjoining bronchus, oesophagus, lung or
pulmonary artery. Partial or complete thrombosis of the aneurysm,
aortic dissection, leak and aortic rupture can also be well demonstrated.
In addition, the mass effect on adjacent structures, status of the lung
parenchyma and pleural cavity is confirmed on reformatted images.
In our case, there were evident features of pulmonary edema in
the right lung parenchyma Left lung parenchyma appeared normal.
The possible explanation of unilateral right sided pulmonary edema
was secondary to compression of the left pulmonary artery. Thus, the
consequence of left to right shunt and elevated pulmonary arterial
pressures manifested as changes involving the right pulmonary artery
and right lung [6].
Cardiac catheterization confirms the fistulous communication
between the aorta and the pulmonary artery, outlining the precise
location and dimension of the fistula. This modality is invasive but
has diagnostic and therapeutic role in managing aorto-pulmonary
arterial fistulas.
Conclusion
Aorto-pulmonary artery fistula is ideally treated surgically and
percutaneous coil embolization has shown favourable outcomes
[7]. Surgeries such as arch replacement and pulmonary arterial
repair may be recommended too. Less invasive therapy including
endovascular stent grafting, combined interventional radiological
and surgical approaches are safer in patients at high risk for surgery
[8-10] The occurrence of aorto-pulmonary fistulas remains rare, and
those caused due to ruptured arch of aorta aneurysms are exceedingly
rare at 4% incidence of all cases reported [11].
References
Citation
Sayed S, Katiyar G, Mulla M, Kumar P, Desai M. Spontaneous Aorto-Pulmonary Artery Fistula Secondary to Ruptured Aortic Arch Aneurysm Presenting as Acute High Output Cardiac Failure. Indian J Appl Radiol. 2025;11(1): 209.