Case Report
Percutaneous Trans-Hepatic Embolization of Peristomal Variceal Bleed in Patient with Recto-sigmoidal Carcinoma with Liver metastasis and Portal Hypertension
Sayed S* and Kumar P
Department of Radiodiagnosis and Interventional Radiology,Goa Medical College and Hospital, Goa, India
*Corresponding author:Shoaib Sayed, Department of Radiodiagnosis and Interventional Radiology, Goa Medical College and Hospital, Goa, India. E-mail Id: shoaibsayed2699@yahoo.com
Copyright: © 2025 Sayed S, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article Information:Submission: 25/11/2024; Accepted: 06/01/2025; Published: 10/01/2025
Abstract
Variceal bleeds in the upper gastro-intestinal tract have been commonly described in cases of raised portal hypertension but ectopic peristomal varices are a rare entity and can have life threatening complications and high mortality. Here, we describe a known case of recto-sigmoidal carcinoma with a palliative sigmoidal stoma who presented with massive bleeding from the stoma site and was treated by percutaneous trans-hepatic variceal embolization
Introduction
Upper GI bleed is a common entity seen regularly in day-today
surgical clinical practice and is dealt with medical management
first via fluids and drugs such as Terlipressin and once the patient
is stable, endoscopic banding is carried out. Peristomal varices are
a rare entity and there is no established guideline for their control
as they tend to be more chronic than hemorrhagic, and now with
the advent of endovascular procedures and improved imaging
modalities, trans hepatic embolization is coming up as the treatment
of choice where transjugular intrahepatic portosystemic shunt (TIPS)
is contraindicated.
Case Presentation
A 39-year-old male, who is a known case of recto-sigmoidal
carcinoma operated in November of 2021 with anterior resection
and a palliative sigmoidal stoma presented to the Emergency
Department (ED) of our hospital with severe stomal site bleeding.
Patient had noticed small streaks of blood one day prior but on the
day of presentation had severe bleeding and passing of blood clots
along with stool from the stoma site. Patient gave history of similar
episodes in the recent past for which he was admitted but managed
conservatively as the bleeding was minimal. There was no history of
fever, trauma to stoma site or per rectal bleeding. Past history was
significant for recto-sigmoidal carcinoma with metastasis to liver, for
which anterior resection was done and sigmoidal stoma was created,
10 cycles of chemotherapy was received. On general examination, the
patient had pallor, no icterus, clubbing, cyanosis, or lymphadenopathy
was noted. The patient had a pulse rate of 96/min, with a blood
pressure of 110/60 mmHg. The patient was conscious and oriented.
Examination of the abdomen revealed a soft, non-tender abdomen
with gross ascites present. The stomal site had blood clots present.
Multi-phase contrast enhanced tomography scan (CECT)
abdomen was done which showed multiple metastatic lesions in the
liver. Few of the lesions had calcific foci with in them [Figure 1a].
There is bunch of vessels seen in the vicinity of the stoma with afferent
from the inferior mesenteric vein (IMV) [Figure 1b] suggestive
ofperistomalvarices.
Given the history of metastasis to liver, recurrence of episodic
bleeding from stoma site which is progressively increasing in severity,
and deranged liver function tests, after discussion with the surgical
team, it was decided that a percutaneous transhepatic embolization
of the variceal bleeding site would be carried out.
The patient was shifted to the Interventional Radiology Cathlab.
Under strict aseptic precautions with the help of USG guidance the
segment III branch of the left portal vein was punctured with the
help of a micro-puncture set and a 6F sheath was placed. With the
help of a 5F Picard catheter, a contrast run of the IMV was taken
which showed large peri-stomal varices with afferent from the
inferior mesenteric vein and efferent in the superficial epigastric
veins [Figure 2a,2b]. With the help of a 2.7F progret catheter
and 25% 2mL glue, embolization of the varices was done. Post
embolization, complete obliteration of peri-stomal varices were seen
[Figure 2c,2d]. The hepatic parenchymal tract was embolized
with the help of 25% glue.
2000IU of heparin was given during the procedure. No
complications were noted during or after the procedure. There was
no bleeding noted from the peri-stomal site and the patient was
discharged on post procedure day 2 in stable condition.
Discussion
Variceal bleeding due to portal hypertension occurs mostly in
the upper gastrointestinal tract and episodes of hemorrhagic ectopic
variceal bleeding have been seen to occur rarely [1]. Only 5% of total
variceal bleeds have been reported to be ectopic in nature, and an
exceedingly small population has been reported to have peri-stomal
bleed [2]. These bleeders tend to be chronic and rarely hemorrhagic.
A multimodality approach using Ultrasound and CECT abdomen
can be used to localize the site of the bleeding. Harding et al [7] have
described the causes of portal hypertension in cases of liver metastasis
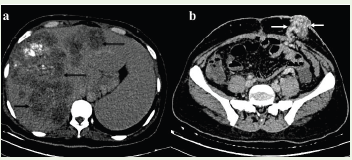
(b) lower abdomen axial section image showing multiple tortuous vessels (white arrows) around the stoma suggestive of peri-stomal varices.
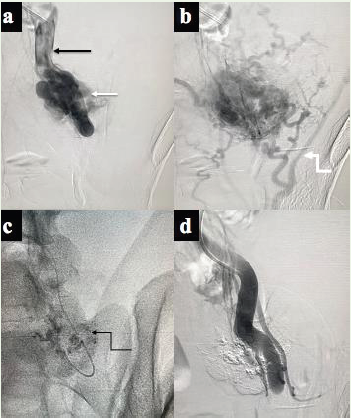
(b) DSA image showing efferent superficial epigastric veins (curved white arrow).
(c) Fluros copy image showing deposition of the 25% N- butyl cyanoacrylate (Glue) in the varices (curved black arrow).
(d) DSA image showing non- visualization of varices suggestive of complete obliteration of the varices post embolization.
to be due to sinusoidal damage and fibrosis. These patients can be
taken up for transjugular intrahepatic portosystemic shunts (TIPS)
but TIPS procedure done in patients with deranged liver functions
can lead to higher occurrence of hepatic encephalopathy. There is
no standard of care established in such patients especially presenting
in an acute setting but endovascular embolization using coil or glue
remains a safe and effective method as described by Yao et al[3]. After
endovascular embolization in an acute setting, TIPS can be performed
concurrently in patients who are ideal candidates [4,5]. Various
methods of embolization exist including glue embolization, gelfoam
embolization or coil embolization [6,7]. Although coil embolization’s
have been found to be effective in controlling major bleeds in an
acute setting, they have not managed to prevent recurrence of bleeds
as described by Toumeh et al [8]. A combination of sclerotherapy and
coil embolization has been found to be more effective in preventing
recurrence. Risks of the procedure include bleeding from liver
parenchyma and embolization of sclerosing material into the portal
vein for which caution has to be taken.
Conclusion
Peri-stomal varices are a rare entity which can be managed
well in a percutaneous transhepaticemboliztion setting along with
sclerotherapy and coilingforming part of the embolization modality.
It is in fact the most preferred treatment option currently in cases
where TIPS is contraindicated.
References
Citation
Sayed S, Kumar P. Percutaneous Trans-Hepatic Embolization of Peristomal Variceal Bleed in Patient with Recto-sigmoidal Carcinoma with Liver metastasis and Portal Hypertension. Indian J Appl Radiol. 2025;11(1): 206.