Case Report
Endovascular Closure of Complex Ascending Aortic Pseudoaneurysm after Aortic Valve Replacement Surgery: “Diffusing the Ticking Bomb”
Sayed S*, Kumar P and Sardessai S
Department of Radiodiagnosis and Interventional Radiology, Goa Medical College and Hospital, Goa, India
*Corresponding author:Dr. Shoaib Sayed, Department of Radiodiagnosis and Interventional Radiology, Goa Medical College and Hospital, Goa, India E-mail Id:shoaibsayed2699@yahoo.com
Copyright: © 2025 Sayed S, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article Information:Submission: 13/11/2024; Accepted: 24/12/2024; Published: 03/01/2025
Abstract
Ascending aortic pseudoaneurysms are rare, life-threatening complication of cardiac surgery, trauma, or infection. They’re predisposed to rupture and distal embolization. Surgical repair of pseudoaneurysms is often considered but is associated with high mortality and morbidity. Alternatively, endovascular closure may be an effective treatment in selected patients, especially in elderly and those with high morbidity where open surgery is not an option. This case emphasizes on the use of multimodality imaging approach for planning and the use of minimally invasive interventional techniques to treat such complex diseases.
Abbreviation:CTA: Computed Tomography Angiogram; TEE: Trans-Esophageal Echocardiography
Introduction
Ascending aortic aneurysms are rare pathologies which if left
untreated will eventually be fatal, the time factor being extremely
crucial. Thus timely diagnosis with accurate imaging modalities along
with interventional methods being deployed is paramount to good
case outcome. With advanced age and co-morbidities, open surgery is
not advisable and that is where endovascular intervention comes into
play and is evolving to become to first line of treatment in all aortic
aneurysms irrespective of size and location. The minimally invasive
nature along with shorter hospital stay and better prognosis all play in
favour of endovascular intervention over open surgery.
Case presentation
56-year-old female presented to the emergency department
(ED) of our hospital with a history of chest pain, breathlessness
and swelling of the chest wall from the last one month. Pain and
breathlessness was increasing in severity progressively. There was no
history of fever, palpitation, weight loss or pus discharging sinus on the
chest wall. Patient gave a significant past medical history stating that
she underwent an aortic valve replacement surgery 9 months ago for a
severely calcified aortic stenosis. She is a newly diagnosed case of Type
I diabetes mellitus, a known hypertensive and has hypothyroidism
and is on treatment for the same. On general examination, her pulse
was 98/min, blood pressure was 130/80 mmHg. She was conscious,
oriented and had no focal neurological deficits. Local examination
findings. Examination of her respiratory system revealed bilaterally
clear lung fields on auscultation. Auscultation of the cardiovascular
system revealed a click, with no murmurs. Per abdomen examination
revealed a soft non-tender abdomen. There was no pallor, icterus,
clubbing, cyanosis, lymphadenopathy or edema present.
Chest X-ray showed mediastinal widening with moderate
cardiomegaly (cardio-thoracic ratio>0.5). Prosthetic aortic valve was
seen in situ and midline sternal sutures were noted.
Trans-thoracic echocardiography (TTE) showed prosthetic
aortic valve in situ and the left ventricular ejection was normal
(~60%). Emergency non-contrast computed tomography (CT)
scan showed an ill-defined hyper dense collection in the anterior
mediastinum in retrosternal location. This collection was extending
medially indenting and displacing the mediastinal vessels, mainly
the ascending aorta and main pulmonary artery towards left side.
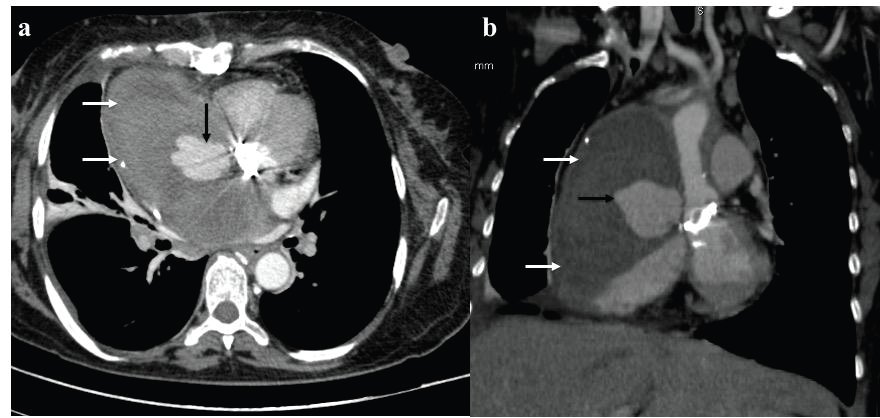
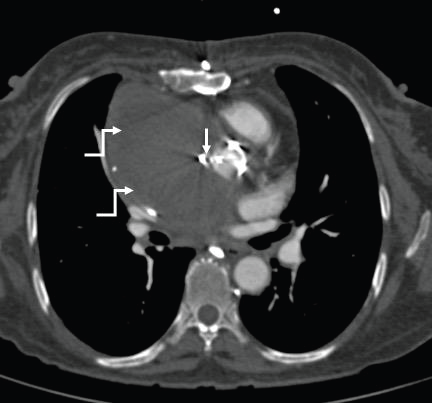
Contrast enhanced CT aortogramwas done which showed pseudo
aneurysm measuring2.9 x 3.4x 3.7cm likely arising from the right
lateral wall of the ascending aorta at the level of prosthetic aortic
valve [Figure 1]. Due to beam hardening effect of the prosthetic
aortic valve, the neck of the pseudo-aneurysm couldn’t be delineated.
This pseudo aneurysm was surrounded by a large hematoma
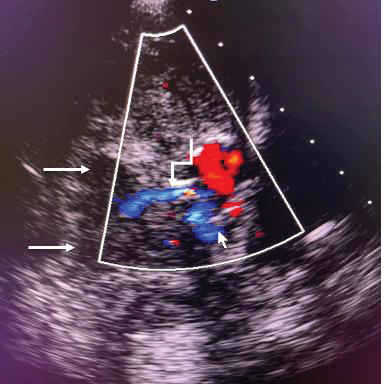
~10x6.6x10.2 cm (AP x TR × SI). Trans-esophageal echocardiography
confirmed the TTE finding. There was a narrow jet (~2 mm)
seen extending into the pseudo-aneurysm [Figure 2]. Given her
fragile general health condition and history of prior surgery, after
multi-disciplinary meeting involving CTVS surgeon, cardiologist and
interventional radiologist, endovascular approach was undertaken
with open surgery as backup. The patient was brought to the Cathlab
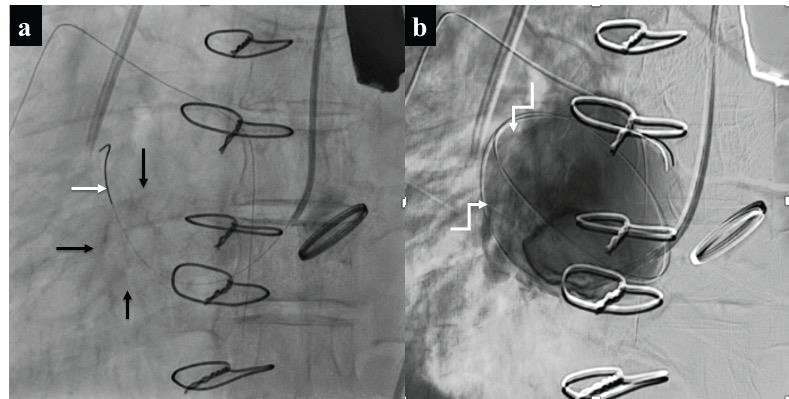
and placed under general anaesthesia. Aortography was performed
with the help of 5F pigtail catheter which showed a small jet of contrast
coming from the right lateral wall of ascending aorta (just above the
aortic valve level) filling the pseudo-aneurysm sac. The rent in the
ascending aortic wall was selectively engaged with the help of 5F- 35
Judkin’s right catheter and 0.014 run-through coronary support wire
was passed in the pseudo-aneurysm sac. On run-through wire and on
2x12 mm coronary balloon catheter was tracked in the aneurysm
sac. Injection through the catheter demonstrated opacification of
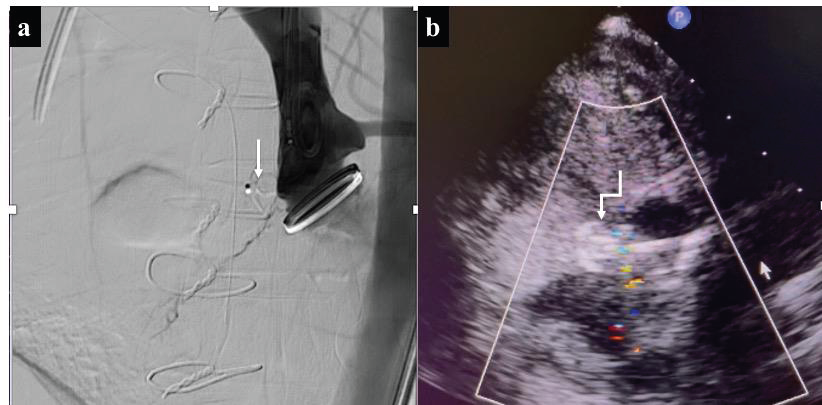
the pseudoaneurysm sac [Figure 3]. A 4x6 mm Amplatzer duct
occluder type- II (AGA medical corporation, Plymouth, MN,
USA) was successfully deployed across the rent. Repeat TEE and
ascending aortography showed a well- seated device with no evidence
of filling of pseudo aneurysm sac [Figure 4a, 4b]. The post
procedure course was uneventful and she was discharged by the
2nd post procedure day. Post procedure follow up after one month
suggested that the patient was doing fine with no chest pain and
no breathlessness. Follow up CECT aortogram was done which
showed complete thrombosis of the pseudo aneurysm and there was
40% reduction in the size of mediastinal hematoma [Figure 5].
Discussion
Most patients with thoracic aneurysm present with symptoms of
chest pain, heart failure or symptoms related to sepsis. The common
aetiologies are atherosclerosis [1], genetic conditions, blood vessel
inflammation, irregular aortic valve, untreated infections, trauma and
previous cardiac surgeries as described by Razzouk et al [2]. Patients
usually present with complaints of dyspnoea, chest pain or mass
effect symptoms such as hoarseness, stridor, or pulsatile swelling [3]
as was seen in our case report. Patients who have undergone surgery
will usually present within 2 years post surgery but longer periods
have been documented too [4]. Trauma during open procedures
can contribute up to 30% in development of pseudo aneurysms thus
making it a major etiological factor. The decision to intervene can
depend on size of aneurysm or impending rupture. Open procedures
are preferred in cases with proximity to root of aorta, but here, owing
to age and previous history of aortic valve replacement, an open
procedure was not warranted, which makes it even more challenging.
Endo vascular repair has emerged as a minimally invasive approach
to aortic pathologies and can be a precedent for all forms of aortic
aneurysm treatment irrespective of location or size. Successful device
closure post-surgical trauma induced pseudoaneurysm has been
described by Petrov4and Kondoleon [5]. CTA and MRA are currently
the preferred modalities of diagnosis and TEE helps assess the extent
of aneurysm and in planning the procedure. Pseudoaneurysms
which fit the criteria, even if asymptomatic, should be considered for
repair, as they have a chance of rupture later in life. Device closure
by endovascular means is emerging as the preferred treatment
modality due to significant mortality associated with open surgery
procedures owing to rupture and other intra-op complications [5].
Open procedures are also extremely invasive which not only give
rise to chance of post-op complications like sepsis but also increase
the in-patient hospital admission times. Endovascular device closure
has come up as a brilliant modality to deal with vessel pathologies
and as discussed, it could be deployed to deal with a large aneurysm
with narrow neck in aselective sub-group of patients. Device closure
of a complex aortic pseudo-aneurysm is feasible and safe. However,
lifelong follow-up is needed to determine the late results of the same.
This procedure could be done in an elderly patient without any
significant complication and a short hospital stay which is a marvel
and milestone of interventional radiology. In conclusion, we described
a case of an ascending aortic pseudoaneurysm, which was diagnosed
9 months after the initial operation (post AVR), in an elderly patient,
and treated within a three week window period. Multimodality
imaging such as CTA and TEE were required in establishing
diagnosis and planning of the procedure. Multidisciplinary approach
is required and open surgery is kept as backup.
Equipment, availability and cost factorial: In this particular
case a 4x6 mm Amplatzer duct occluder type- II (AGA
medical corporation, Plymouth, MN, USA) was used, which has ready
availability and in emergency can be requested from the supplying
companies as well. In different types of other aortic aneurysms,
Medtronics stent grafts are being routinely deployed which are
supplied as emergency equipment depending on patient aorta size and
length of the aneurysm. These have a cost factorial upwards of Rupees
5 lakhs (6000$) and can go all the way up to Rupees 25 lakhs (30000$)
depending on the number of grafts needed and vessels involved. In
various government settings, part cost of the procedure is covered
by the government while the remaining is covered by the patient.
Endovascular stent grafts and plugs are widely available across India
and are either custom made or the nearest available size is used, and
with increasing demand and advancing technology, the price factorial
is becoming more affordable year after year.Endovascular device
closure of arch of aorta aneurysms are being done routinely now in
higher centres where Interventional Radiology and Cardiovascular
Surgery are available in the same institute [6], but the overall incident
of such treatment still remains rare at 0.5% globally [7].
Conclusion
With advancing technology and availability of high-resolution
imaging modalities along with ever evolving interventional
techniques, a large number of aortic aneurysms are being dealt with
endovascular intervention over open surgery and it has reflected
statistically in patient outcome, and duration of hospital stay. Open
surgery associated complications are also bypassed with interventional
techniques and in the coming years it will become the gold standard
of aortic repair, no matter the size or location of the aneurysm.
References
Citation
Sayed S, Kumar P, Sardessai S. Endovascular Closure of Complex Ascending Aortic Pseudoaneurysm after Aortic Valve Replacement Surgery: “Diffusing the Ticking Bomb”. Indian J Appl Radiol. 2025;11(1): 204.