Case Report
A Tale of Two Isolated Pancreatic Masses Mimicking Pancreatic Neoplasm
Duddukuru H1, Vanidassane D2, Pitchaimuthu A3, Singh Naik S4*, and Banu SN5
1,4Department of Radiodiagnosis, MGMCRI, Pondicherry, India
2Department of Medical Oncology, MGMCRI, Pondicherry, India
3Department of Radiodiagnosis, AIIMS, Bhubaneswar, India
5Department of Pathology, MGMCRI, Pondicherry, India
2Department of Medical Oncology, MGMCRI, Pondicherry, India
3Department of Radiodiagnosis, AIIMS, Bhubaneswar, India
5Department of Pathology, MGMCRI, Pondicherry, India
*Corresponding author:Shailendra Singh Naik, Assistant professor, Department of RadiodiagnosisMahatma Gandhi Medical College and Research Institute, Pondicherry, India. Email Id:drnayak1388@gmail.com
Copyright: ©2024 Duddukuru H, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article Information:Submission: 10/04/2024; Accepted: 11/05/2024; Published: 05/06/2024
Abstract
Tuberculosis (TB) is a common disease in developing countries but isolated Pancreatic tuberculosis is an extremely rare entity even in endemic areas. It is often misdiagnosed due to a low index of suspicion and masquerading of its symptoms with more common pancreatic malignancy. The clinical and
radiological features resemble malignancy, making diagnosis a clinical challenge. The definitive diagnosis rests on histologic and bacteriologic evidence of TB. Excellent cure rates are reported with standard anti-tubercular therapy given for 6–12 months. We discuss two cases of pancreatic TB successfully
diagnosed and treated and their relevant literature.
Keywords:Isolated pancreatic TB, Abdominal tuberculosis
Introduction
Pancreatic masses can be benign or malignant. Pancreatic
adenocarcinoma constitutes 85 to 90 percent of all pancreatic
neoplasm, the most common benign pancreatic neoplasm is serous
cystadenoma. Pancreatic tuberculosis is an uncommon form of
extrapulmonary tuberculosis and usually presents with abdominal
pain, jaundice, and constitutional symptoms. It usually occurs as a
complication of miliary TB and immunodeficiency, with isolated
involvement of the pancreas being extremely rare. We present two
cases of pancreatic tuberculosis mimicking pancreatic malignancy.
Here we discuss various clinco-radiological features of pancreatic
tuberculosis with a review of literature.
Case Series
Case 1:
A 42-year-old female presented to our hospital with complaints
of fever, weight loss, epigastric pain, and anorexia. No history of
tuberculosis. She was afebrile, physical examination revealed marked
epigastric tenderness with otherwise unremarkable examination.Case 2:
A 26-year-old young hypertensive male presented to our hospital
with complaints of weight loss, on and off abdominal pain, icterus,
and severe fatigue. No history of tuberculosis. At his initial evaluation
in the ER, he was afebrile with stable vitals, physical examination
revealed icterus and epigastric tenderness.Laboratory Evaluation:
Laboratory evaluation of both patients revealed deranged Liver
enzymes and a negative HIV test. Ca19.9, Serum electrolyte, blood
urea nitrogen, creatinine, bilirubin, amylase, lipase, and chest
radiography were all normal in case 1. Case 2 had total bilirubin
of 5.0 mg/dl and raised liver enzymes. Ultrasound of the abdomen
revealed a hypoechoic mass in the region of the head of the pancreas.
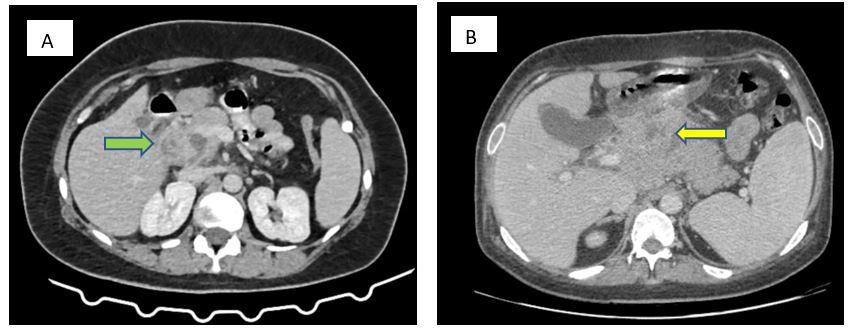
Contrast-enhanced computed tomography of the abdomen revealed
a heterogeneously enhanced diffusely bulky pancreas with ill-defined
necrotic areas, adjacent peripancreatic fat stranding, and loss of fat
plane with the adjacent duodenum. Multiple conglomerate low density
necrotic nodal lesions were noted in the peripancreatic,
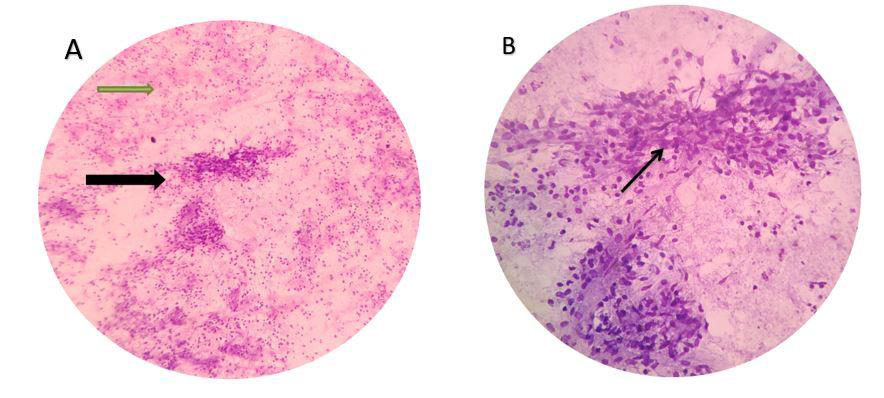
portocaval, and periportal regions. [Figure 1 A,B]The patients underwent ultrasound-guided fine needle aspiration
of the mass for tissue diagnosis. Both cases revealed chronic caseating
granulomatous lesion, and occasional AFB in Ziehl nelson stain
suggestive of Tuberculosis [Figure 2 A,B].
Both were started on anti-tuberculosis treatment (ATT) with
isoniazid (H), rifampicin(R), pyrazinamide (Z), and ethambutol
(E) daily under category I according to The Revised National
Tuberculosis Control Program (RNTCP) -Directly Observed
Treatment Short-course (DOTS) strategy. On follow-up after
two months of treatment, there was a significant improvement in
weight and constitutional symptoms, and they are continuing their
treatment.
Discussion
Abdominal TB comprises 5% of all TB cases and usually involves
the intestinal tract, peritoneum, and lymph nodes. Pancreatic TB
was seen in 4.5% of cases of abdominal TB in a study. [1] Isolated
pancreatic TB is extremely rare. Common risk factors include
immunocompromised states and malignancy in non-endemic
regions. In endemic regions, reactivation of latent TB is the most
common cause. Both of our patients did not have a history of
tuberculosis or immunocompromised states.
The pathogenesis of isolated pancreatic TB is not clear. Pancreatic
secretions and its retroperitoneal location have been postulated
for decreasing the incidence of pancreatic TB. [2] Mechanisms
such as lympho hematogenous dissemination from pulmonary
disease or lymphatic spread of epithelial granulomas formed in the
gastrointestinal tract after ingestion of bacilliare hypothesized.
The common presentation includes abdominal pain, jaundice,
loss of appetite, and loss of weight. These symptoms mimic pancreatic
malignancy making it difficult to suspect TB based on symptoms.
Presence of pulmonary tuberculosis has been reported in 50% of
cases of pancreatic TB, other features also include anemia, raised ESR
and icterus in some cases. Both our cases did not show any evidence
of pulmonary TB, case 2 presentation with icterus, though both had
deranged liver enzymes.
In various series, the pancreatic TB mass presents as a hypoechoic
lesion in Ultrasound.It also helps in evaluation of extra-pancreatic
findings like ascites, omental thickening, etc.[3] The most common CT
abdomen finding of pancreatic TB is a focal mass of low attenuation,
which is difficult to differentiate from pancreatic carcinoma. Majority
of tuberculous pancreatic masses occurred in the head. Other CT
findings include cystic mass, small nodular lesions, pancreatic
calcification, and focal and diffuse enlargement of the pancreas.[4]
Similarity with pancreatic malignancy includes the common
presenting features, imaging with a mass lesion, commonly involves
the head of pancreas. In pancreatic carcinoma, the hypoattenuating
appearance may be due to central necrosis, or because of differential
contrast enhancement by tumor tissue and normal pancreas. In
pancreatic TB, the non-enhancing areas may represent caseating
necrosis or pus. Soft differentiating points include adenocarcinoma
more commonly associated with secondary signs, such as
interruptionof the pancreatic duct, distal pancreatic atrophy, and
mass effect can be seen.
The first step in the diagnosis of pancreatic tuberculosis is a high
index of clinical suspicion especially in individuals residing in
endemic countries. The approach for lesion sampling from the pancreas
should be the same as it is for presumed pancreatic malignancy.
The lesion should be assessed for obtaining tissue diagnosis either
using CT or ultrasound-guided biopsy for microbiological and
histopathological evaluation.
Unlike the diagnosis, the treatment of pancreatic TB is relatively
straight forward. Extrapulmonary TB includes two months of
intensive HRZE followed by 4 months of HR treatment. Most cases of
pancreatic TB respond well to Anti Tuberculous Drugs for duration
of 6 to 12 months in various series, selected cases would require
surgical interventions for obstructive jaundice.
Conclusion
In conclusion, we presented two cases of pancreatic TB presenting
as pancreatic mass. This case report highlights the risk of pancreatic
TB being easily missed, owing to common presenting features. Being
aware of the differential diagnosis will help in early diagnosis. It
avoids unnecessary diagnostic or therapeutic delay, in a very treatable
extra pulmonary TB which has excellent outcomes.
Consent:Patient’s consent has been obtained.
References
Citation
Duddukuru H, Vanidassane D, Pitchaimuthu A, Singh Naik S, Banu SN. A Tale of Two isolated Pancreatic Masses Mimicking Pancreatic Neoplasm. Indian J Appl Radiol. 2024;10(1): 197.