Case Report
A Rare Case of Arteriovenous Malformation: Pelvic Wall AVM in Male
Parvin H*, Hazra S, Dutta A and Ali W
Department of Clinical Imaging and Interventional Radiology, Apollo Multispecialty Hospitals, 700054 Kolkata, West Bengal, India
*Corresponding author:Hena Parvin, Department of Clinical Imaging and Interventional Radiology, Apollo Multispecialty Hospitals, 700054 Kolkata, West Bengal, India, Email Id: drhena_p@apollohospitals.com
Copyright:© 2024 Parvin H, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article Information:Submission: 04/04/2024; Accepted: 29/05/2024; Published: 05/06/2024
Abstract
Congenital pelvic arteriovenous malformation (AVM) is an uncommon vascular anomaly characterized by direct connection between arteries and veins, encompassing a malformed vascular network, or nidus. Due to its infrequent occurrence and the nonspecific nature of its symptoms, congenital pelvic AVM
in males has been seldom explored. In this case study, we discussed a 64-year-old male who visited the gastroenterology outpatient department at Apollo Multispecialty Hospitals, Kolkata, reporting a mild, dull aching pain on the right side of his abdomen for the past five months. A high-flow pelvic wall AVM was
identified through CECT whole abdomen. Absence of any other contributing pathology indicated congenital origin of AV malformation.
Keywords:Arteriovenous Malformation; Pelvic Wall AVM; Vascular Malformation; Venous Malformation; Interventional Radiology
Abbreviation
AVM: Arteriovenous Malformation; CECT: Contrast Enhanced
Computed Tomography; USG: Ultrasonography; MIP: Maximum
Intensity Projection
Introduction
Arteriovenous malformation (AVM) represents a vascular
anomaly characterized by the connection of arteries and veins through
a nidus of dysplastic vascular channels [1]. Among these, pelvic wall
AVMs are particularly uncommon, with an even rarer occurrence
in male patients [2,3]. The majority of pelvic AVMs arise secondary
to trauma, previous surgeries, or tumours, making congenital pelvic
AVMs in males exceedingly rare [4]. These malformations typically
involve bone and soft tissues of the pelvic wall, draining into the
branches of the internal iliac veins. Over time, as they grow, arteries
and veins from the pelvic organs may also become involved. In
addition to collateral from adjacent visceral branches, pelvic wall
AVMs are usually fed by a multitude of vessels including branches
of pudendal, obturator, and gluteal arteries, potentially reaching
substantial sizes and flow rates.The clinical presentation of pelvic
AVMs is varied and nonspecific [5-8]. Some individuals may remain
asymptomatic, with the diagnosis only made incidentally during
cross-sectional imaging of the pelvis for unrelated reasons.
This case report details a rare presentation of a congenital pelvic
AVM in a male patient, who reported nonspecific symptoms such
as dull aching abdominal pain. A CECT of the whole abdomen
ultimately revealed a high-flow arteriovenous malformation on the
right side of the pelvic wall.
Case Presentation
A 64-year-old male visited the gastroenterology outpatient
department at Apollo Multispecialty Hospitals, Kolkata, reporting
a mild, dull ache on the right side of his abdomen. The pain was
persistent for last five months. An ultrasound of the whole abdomen,
previously performed at an external peripheral centre, showed no
significant findings. Physical examination did not uncover any notable
abnormalities, and his vitals were stable. The patient had a history of
type 2 diabetes mellitus for which he was under medication. He also
mentioned self-administering over-the-counter pain relievers for his
abdominal discomfort, though these did not provide any noticeable
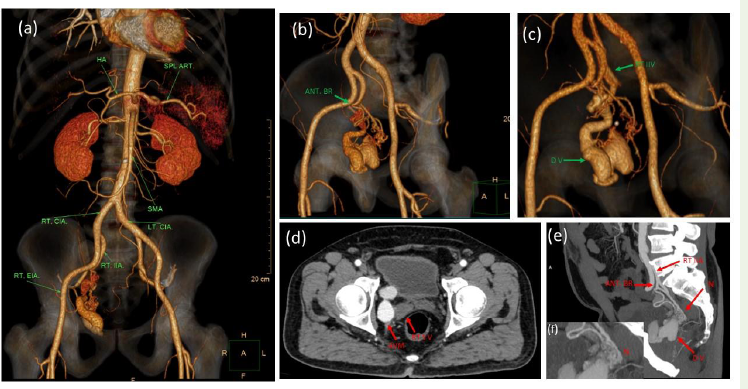
relief. A whole abdomen CECT was advised. It revealed, a high-flow
pelvic arteriovenous malformation on the right side, with an illdefined
nidus just adjacent to the right seminal vesicle. It wasfed by
multiple very small calibre arterial channels arising from the anterior
branch of the right internal iliac artery, with a large dilated, tortuous
draining vein, showing early opacification and ending into the right
internal iliac vein [Figure 1].
Discussion
Pelvic congenital arteriovenous malformations (AVMs) in males
are notably rare. In 2002, Game et al. documented two cases of pelvic
congenital AVMs in male patients and reviewed an additional 15
cases previously reported in the literature, with only a handful more
cases identified since then [9]. We discuss a scarce instance of a male
patient diagnosed with a congenital pelvic AVM via CECT of the
whole abdomen. In AVMs, the nidus, a malformed vascular plexus
formed by remnants of the capillary network, acts as an intermediary
between arterial and venous systems. While AVMs can develop in
any body part, they are most commonly found in the brain, neck,
kidneys, and lungs, with pelvic AVMs, particularly in males, being
exceedingly uncommon [10,11].
The symptoms associated with pelvic AVMs lack specificity and
range from subtle to vivid, potentially leading to lethal outcomes. They
include flank, abdominal, or pelvic pain, hematuria, hemospermia,
impotence, dysuria, and dyspnea due to high-output heart failure,
among others [12,13]. Additionally, foot drop resulting from nerve
compression and lower extremity edema caused by proximal iliac vein
compression have been described [5-8]. The rarity of the condition,
combined with the nonspecific nature of its symptoms, complicates
early clinical diagnosis. Significant indicators of pelvic AVM include
palpating a pulsatile mass and detecting loud or harsh noises upon
physical examination, though deep pelvic AVMs are not palpable.
In contrast to previous literature, few studies show the application
of Doppler and USG is also a potential tool of solid diagnostic value
for congenital pelvic AVM in males [14,15]. In the case we present,
the patient experienced mild, dull aching pain on the right side of
his abdomen for several months. Initial physical examinations and
an ultrasound of the whole abdomen showed no abnormalities. A
CECT of the whole abdomen was performed to exclude any sinister
pathology, revealing a high-flow pelvic arteriovenous malformation,
presumed to be congenital due to the absence of other significant
contributory pathologies.
Treatment for congenital pelvic AVM in males varies based on
the severity of symptoms. Lesions that are asymptomatic or mildly
symptomatic may not require intervention. In this case, the patient
was presented with various treatment options if his symptoms would
intensify. Treatments for AVM in males have included ligation
of afferent arteries, lesion excision, embolization, and surgical
approaches. Surgical intervention often leads to complications such
as haemorrhage, damage to adjacent organs, and recurrence, making
it less favourable. Embolization, offering lower morbidity, mortality,
and invasiveness, is preferred.Slow-flow VMs (venous and lymphatic
malformations) are often treated by sclera therapy [16-18].Our
patient was offered embolization under fluoroscopy guidance as the
treatment modality. However, he opted against definitive treatment,
choosing instead a conservative ‘wait and watch’ approach.
Conclusion
Congenital pelvic arteriovenous malformation (AVM) is an
uncommon vascular anomaly characterized by direct connections
between arteries and veins, encompassing a malformed vascular
network, or nidus. Only a few cases are reported in males. This case
report details presentation of a congenital pelvic AVM in a 64-yearold
male patient, who reported nonspecific symptoms such as dull
aching abdominal pain. A CECT of the whole abdomen ultimately
revealed a high-flow arteriovenous malformation on the right side of
the pelvic wall.
Teaching points:
•Congenital pelvic wall arteriovenous malformation is a rare
entity, rarer in males.• The symptoms associated with pelvic AVMs are mostly nonspecific and include flank, abdominal, or pelvic pain, haematuria, hemospermia, impotence, dysuria, dyspnoea due to high-output heart failure, foot drop, and lower extremity edema.
• Sometimes it’s an incidental finding.
• Treatment for congenital pelvic AVM in males varies based on the severity of symptoms.
Acknowledgement
The authors would like to thank Dr. Usha Goenka, director
and head, of the department of clinical imaging and interventional
radiology in Apollo multispecialty hospitals, for reviewing the
case and Mr. Susil Das, senior CT technologist, for volumetric
reformation of the CECT images. Author would also like to thank Dr.
Mofasser Mallick, Group leader scientist, KIT, Germany for editing
and reviewing the report.
Declaration of patient consent:
The authors certify that they have obtained all appropriate patient
consent.References
Citation
Parvin H, Hazra S, Dutta A, Ali W. A Rare Case of Arteriovenous Malformation: Pelvic Wall AVM in Male. Indian J Appl Radiol. 2024;10(1): 196.