Case Report
Pseudomeningocele: The Post-Laminectomy Complication Revealed Through Imaging
Abhighna G, Anughna G, Naveen D*, Vishwapremraj DR, Vinodhkumar K and Mallikarjunappa B
Department of Radiodiagnosis, Sapthagiri Institute of Medical Sciences and Research Centre, Bangalore, India
*Corresponding author:Naveen D, Department of Radiodiagnosis, Sapthagiri Institute of Medical Sciences and Research Centre, Bangalore, India. Email id: drnaveen4@yahoo.com
Copyright: © 2024 Abhighna G, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article Information:Submission: 10/04/2024; Accepted: 08/05/2024; Published: 10/05/2024
Abstract
Pseudomeningocele, an abnormal accumulation of cerebrospinal fluid (CSF) outside the dural-arachnoid layer, is primarily iatrogenic and can occur following spinal surgery, particularly after incidental durotomy. While it is often asymptomatic, it can present with various symptoms. The exact incidence is
uncertain but is estimated at 0.07–2% of lumbar surgeries. Recognizing and managing pseudomeningoceles is essential to preventing complications such as spinal cord compression and nerve root herniation. Here we describe a case of a giant pseudomeningocele that developed as a complication following
post-laminectomy with discectomy.
Keywords:Pseudomeningocele; Post-Laminectomy; Meningocele
Introduction
A pseudomeningocele is an abnormal collection of cerebrospinal
fluid (CSF) outside the dural-arachnoid layer, which is usually
caused by a communication between the dura-arachnoid layer
and extradural tissue. Despite being frequently asymptomatic,
pseudomeningoceles can present with a variety of symptoms,
including postural headaches, back pain, muscular spasms, radicular
syndromes, tinnitus, photophobia, neck stiffness, and gastrointestinal
symptoms like nausea and vomiting.[1] Determining the exact
incidence of post-laminectomy pseudomeningoceles presents
challenges, largely due to their often-asymptomatic nature, resulting
in many cases going unnoticed. However, they are reported to
occur in approximately 0.07% to 2% of lumbar laminectomies and
discectomies. This prevalence is higher in lumbar surgeries due to
the elevated intrathecal pressure in this region and the frequency of
procedures performed there. [2]
Even though they are more uncommon, pseudomeningoceles
can cause complications such spinal cord compression, nerve root
herniation, and radicular discomfort. This emphasizes how crucial
it is to recognize and manage these kinds of cases appropriately. [3]
We report a case of giant pseudomeningocele, which developed as a
consequence of a laminectomy and discectomy.
Case Report
A 43-year-old male patient presented to the neurosurgery
department with complaints of low backache and bilateral lower limb
pain for three weeks, which worsened over the past week. He also
reported a severe headache for the past week. The patient had a history
of re-exploration of L3 laminectomy with discectomy for recurrent
L3-L4 disc prolapse two months prior. On examination, focal swelling
was noted in the spine. An MRI of the spine was recommended to rule
out post-surgical complications, such as CSF leaks. The MRI [Figure 1]
revealed a large, relatively well-defined cystic lesion with CSF intensity
measuring approximately 9.0 x 8.1 x 11.4 cm (AP x TR x CC) in the
posterior aspect of the back from the L2-L5 disc levels and extending
inferiorly. This lesion communicated anteriorly with the midline and
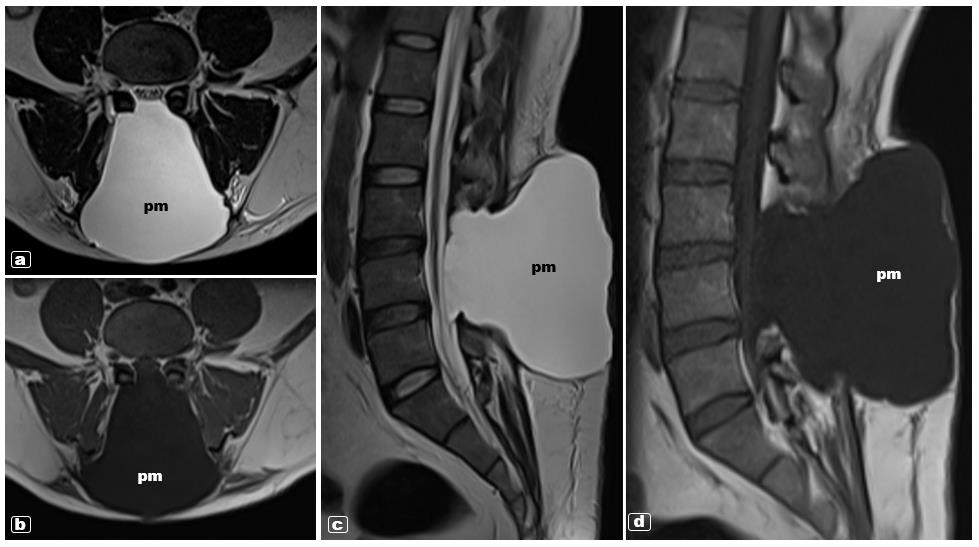
right side of the dorsal thecal sac at the L3 and L4 vertebral levels, and
posteriorly, it was limited by the skin surface. Pedicle screws were
noted at the L3 and L4 vertebrae, and the spinous processes of L3 and
L4 was not visualized. These imaging findings were suggestive of a
post-operative giant pseudo-meningocele. Subsequently, the patient
underwent surgical exploration and repair. The procedure involved
debridement and closure of the dural defect. The patient had a good
postoperative recovery.
Discussion
Pseudomeningoceles can arise through two primary mechanisms.
In one scenario, there is a chronic cerebrospinal fluid (CSF) leaking
due to a tear in both the dura and arachnoid layers. A pseudocyst
develops as a consequence of this persistent leakage resulting
from an aberrant connective tissue response in the paraspinal
region. The second mechanism results in the development of a
pseudomeningocele lined with arachnoid tissue as intact arachnoid
tissue protrudes through a dural defect created during surgery. The
formation of pseudomeningocele is primarily brought about by the
first mechanism, however it is also occasionally caused by the second
mechanism, that results in an arachnoid-lined pseudomeningocele.
[3]
In 1946, Hyndman and Gerber first reported the existence of
postoperative pseudomeningocele in a survey done on extradural
cysts. [3,4] Other terms like “meningocele spurious,” “pseudocyst,” or
“false cyst” have also been used to refer to pseudomeningoceles. While
resembling a meningocele by containing CSF, a pseudomeningocele
is distinguished by its cyst wall, which is made of scar tissue rather
than a meningeal membrane.[3,5]
If a surgical procedure causes an accidental tear in the dura but
leaves the arachnoid intact, the arachnoid may herniate through the
defect into the epidural space, forming an extradural cyst. However,
it is more common for both the dura and arachnoid to tear, leading
to the leakage of cerebrospinal fluid (CSF) into the nearby paraspinal
soft tissues. Initially, the leaked CSF is easily absorbed.[3]However, as
time progresses, a fibrous reaction develops, impeding reabsorption
and causing CSF to accumulate in the paravertebral tissues, eventually
resulting in the formation of a pseudomeningocele. The CSF may
then be resorbed or encapsulated by fibrous tissue, resulting in the
development of a pseudomeningocele. In some situations, nerve
roots may protrude into the pseudomeningocele cavity. [3]
Pseudomeningoceles larger than 5 cm are commonly referred to as
“large,” and those larger than 8 cm are called “giant”. Some cases have
shown spontaneous resolution of giant pseudomeningoceles. This
resolution is expected to occur gradually, probably as a result of the slow
healing of the dural tear and gradual reabsorption of extradural CSF.[1]
The diagnosis of pseudomeningocele is commonly established
using magnetic resonance imaging (MRI), which reveals
characteristic imaging features. Specifically, on T1-weighted images,
pseudomeningoceles display low signal intensity, while on T2-
weighted images, they demonstrate high signal intensity. [6]
Management of pseudomeningocele varies depending on
clinical presentation. Asymptomatic cases can often be managed
conservatively, with reports indicating spontaneous resolution
in some cases of giant pseudomeningoceles. Persistent CSF leaks
typically necessitate surgical intervention. The surgical approach
involves repairing the dural defect and closing the dura-arachnoid
layer. In certain instances, postoperative subarachnoid drainage may
be employed to minimize the risk of recurrence.[2,7,8]
Conclusion
Pseudomeningocele is a rare but significant complication of
spinal surgery, primarily resulting from iatrogenic causes. While
often asymptomatic, it can present with various symptoms and may
require surgical intervention for persistent CSF leaks. Management
strategies should be tailored to the individual patient, with careful
consideration of the clinical presentation and imaging findings. Early
recognition and appropriate management are essential for optimizing
outcomes in patients with pseudomeningocele.
References
Citation
Abhighna G, Anughna G, Naveen D, Vishwapremraj DR, Vinodhkumar K, et al. Pseudomeningocele: The Post-Laminectomy Complication Revealed Through Imaging. Indian J Appl Radiol. 2024;10(1): 195.