Pictorial Essay
Cecal Volvulus: Retrospective Analysis of CT Evaluation in the Emergency Teleradiology Setting with a Pictorial Review of the Salient Features
Rao P1*, Kalyanpur A2 and Menon A3
1Senior Scientific Officer, Image Core Lab, Whitefield, Bangalore, India
2Chief Radiologist, Teleradiology Solutions, Whitefield, Bangalore, India
3Consultant Radiologist, Image Core Lab, Whitefield, Bangalore, India
2Chief Radiologist, Teleradiology Solutions, Whitefield, Bangalore, India
3Consultant Radiologist, Image Core Lab, Whitefield, Bangalore, India
*Corresponding author:Pallavi Rao, Senior Scientific Officer, Image Core Lab, Whitefield, Bangalore, India. E-mail Id:dr.pallavirao.radiology@gmail.com
Copyright: © 2024Rao P, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Article Information:Submission: 21/03/2024; Accepted: 26/04/2024; Published: 30/04/2024
Abstract
Cecal volvulus is a torsion of the cecum around its own mesentery and accounts for 30% of all colonic volvulus. It is predisposed to by a developmental failure of peritoneal fixation, allowing the proximal colon to be free and mobile.
Materials and Methods:This study is a retrospective evaluation of 80 contrast computed tomography (CT) abdomen and pelvis studies acquired in an emergency teleradiology setting with a diagnosis of Cecal volvulus on the communicated report. The study images selected using keyword search were analysed by four expert radiologists to document salient imaging features, unusual findings, and complications in Cecal volvulus on CT abdomen and pelvis images. The results were analysed to compile a pictorial review along with a statistical compilation.
Results:Our study demonstrated that a dilated and displaced cecum with a whirl sign was the most common imaging findings seen in 97.5% and 95% of the patients diagnosed with Cecal volvulus. Cecal wall thickening was seen in 11.2% of the studies, associated small bowel obstruction was seen in 32.5% of the studies and a beak sign was demonstrated in 48.7% of the studies. Mesenteric oedema was seen in 20% of the patients, while uncommon findings (<5%) included pneumatosis, bowel perforation, and intraluminal haemorrhage.
Conclusion:Cecal volvulus is an acute abdominal emergency requiring expeditious diagnosis. Identification of an abnormally located dilated cecum with a whirl sign on CT is helpful to alert the referring physician of this entity. Early diagnosis of Cecal Volvulus can prevent the occurrence of bowel strangulation, gangrene, perforation, and peritonitis.
Materials and Methods:This study is a retrospective evaluation of 80 contrast computed tomography (CT) abdomen and pelvis studies acquired in an emergency teleradiology setting with a diagnosis of Cecal volvulus on the communicated report. The study images selected using keyword search were analysed by four expert radiologists to document salient imaging features, unusual findings, and complications in Cecal volvulus on CT abdomen and pelvis images. The results were analysed to compile a pictorial review along with a statistical compilation.
Results:Our study demonstrated that a dilated and displaced cecum with a whirl sign was the most common imaging findings seen in 97.5% and 95% of the patients diagnosed with Cecal volvulus. Cecal wall thickening was seen in 11.2% of the studies, associated small bowel obstruction was seen in 32.5% of the studies and a beak sign was demonstrated in 48.7% of the studies. Mesenteric oedema was seen in 20% of the patients, while uncommon findings (<5%) included pneumatosis, bowel perforation, and intraluminal haemorrhage.
Conclusion:Cecal volvulus is an acute abdominal emergency requiring expeditious diagnosis. Identification of an abnormally located dilated cecum with a whirl sign on CT is helpful to alert the referring physician of this entity. Early diagnosis of Cecal Volvulus can prevent the occurrence of bowel strangulation, gangrene, perforation, and peritonitis.
Keywords:Cecal Volvulus; Whirl Sign; Cecal Dilatation
Introduction
Cecal volvulus is one of the causes of acute closed-loop intestinal
obstruction where the cecum twists around its mesentery [1,2].
There has been an increase in its incidence in recent years, especially
in individuals with prior abdominal surgical intervention [3], or a
developmental failure of peritoneal fixation, allowing the proximal
colon to be unusually mobile. Restriction of the bowel at a fixed
point within the abdomen serves as a fulcrum for rotation, such as a
neoplastic mass, adhesion, or scarring [2,4]. The clinical presentation
of Cecal volvulus is often vague and restricted to nonspecific
intermittent acute abdominal pain/distension, constipation, nausea,
and vomiting [5,7]. This makes the diagnosis hard and a failure of
timely diagnosis can result in Cecal ischemia, perforation, sepsis, and
death [7,13].
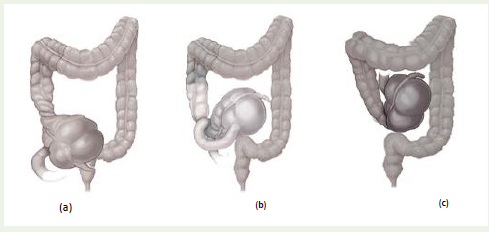
Cecal Volvulus is classified into 3 types::
Type 1:Cecum twists in the axial plane, rotating clockwise
and counter-clockwise in a long axis, appearing in the RLQ (Right
Lumbar Quadrant).Type 2:Loop type, twisting or torsion of the cecum and terminal ileum to an ectopic location (typically left upper quadrant) with relocation in an inverted orientation, commonly counter-clockwise twist
Type 3:Cecal bascule: cecum folds anteriorly or posteriorly without any torsion, seen as dilated loop in the mid abdomen [5-10].
Aims and Objectives
The purpose of this study is to evaluate salient imaging features,
complications, and unusual findings in Cecal Volvulus on CT
Abdomen and pelvis.
Materials and Methods
We performed a retrospective compilation through a keyword
search of reports on our Radiology information system database that
contained CT abdomen and pelvis studies with/without contrast
from January 2019- December 2022. We qualified 80 studies with
a diagnosis of Cecal volvulus on the teleradiology report conveyed
by our institution. These studies were independently analysed after
anonymization and removal of earlier Radiological interpretations,
by four expert radiologists with an experience ranging from 13 to 25
years. We used diagnostic grade monitors with an in-house PACS
system and FDA certified image viewer “RADSpa” for image analysis.
A response template questionnaire was prepared to document
presence or absence of various imaging features of Cecal volvulus. The
imaging features of Cecal volvulus in our list included the position of
cecum, Whirl Sign, Cecal wall thickening, pneumatosis, small bowel
obstruction/distension, presence of free air, beak sign, Cecal diameter
[2, 15]. Mesenteric oedema, mesenteric fat stranding, distal colonic
compression. The results were analysed to show the frequency of each
finding in our series. Example studies with each type of radiological
feature were parallelly compiled in a pictorial review.
Results
Our study demonstrated that a dilated and displaced cecum
with Whirl sign was the most common imaging finding seen in
97.5% and 95% of the patients diagnosed with Cecal volvulus. Cecal
wall thickening, small bowel obstruction, beak sign and mesenteric
oedema were seen in 11.2%, 32.5%, 48.7% and 20% of the studies.
Rare findings (<5%) included pneumatosis, bowel perforation, and
intraluminal haemorrhage.
Discussion
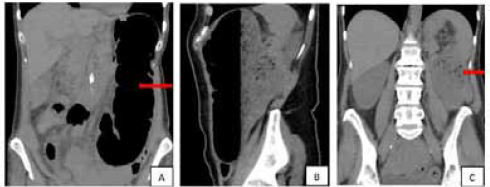
This pictorial review demonstrates findings helpful in the
diagnosis of Cecal volvulus. Displaced cecum outside the right lower
quadrant is one of the key features of Cecal volvulus. In the Axial
type I torsion, cecum remains in the right lower quadrant, in loop
type II torsion, Cecum occupies the left upper quadrant and the Cecal
bascule is seen in the mid-central abdomen [11].
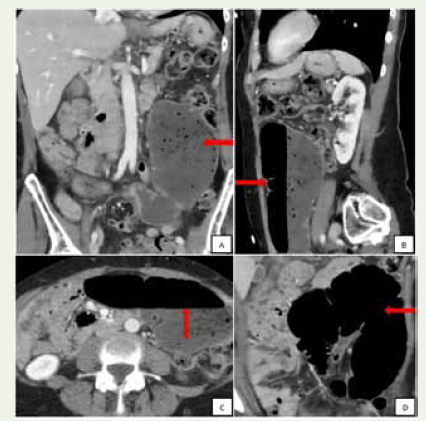
“Bascule” is a French term for seesaw [12]. It is a condition where
the distended cecum folds on itself anteriorly or supero-medial
without torsion possibly secondary to congenital adhesions [14].
CT may demonstrate a dilated cecum ectopically located in the midabdomen
with absent Whirl sign [15,17].
Whirl sign occurs when the afferent and efferent loops of the
Cecal volvulus rotate around a fixed point causing the mesentery to
Cases with classic features in our series:
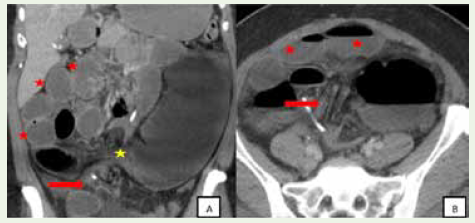
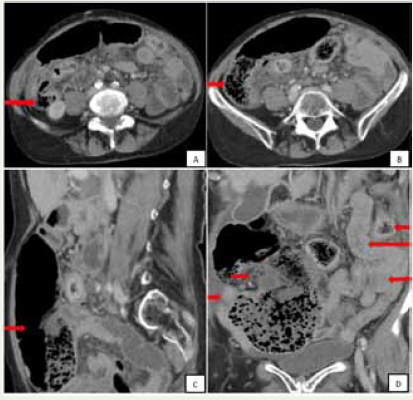
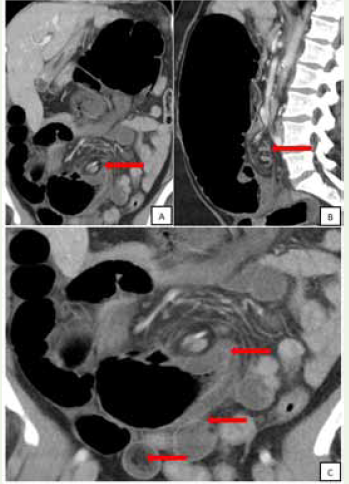
twist in the axis of rotation. The mesenteric vessels create a swirling
appearance with fat stranding in the mesocolon similar to a whirlpool.
This sign is best-observed perpendicular to axis of the volvulus and
may need an evaluation of reformatted images in various planes [18,20]. Beak sign is a smooth tapering or cut-off at the efferent limb
of the obstruction at the site of the twist. It may be seen in CT and
barium/ Bowel contrast studies [16,19].
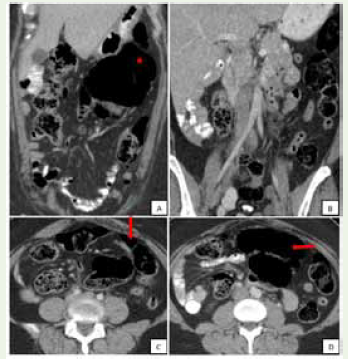
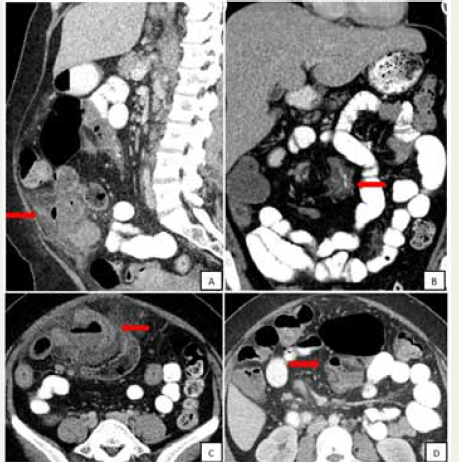
Complicated Cecal volvulus with small bowel obstruction was
seen in 32.5% of the cases. Bowel wall thickening, pneumatosis,
free air, abscess, bowel ischemia, and sepsis were indicators of
complications. Dilated and displaced cecum in abnormal location
was seen in all cases, Whirl sign (95%), distal colon decompression
(53.7%) and Beak sign (48.7%) were the most classic findings of Cecal
volvulus.
Conclusion
Cecal volvulus is an acute abdominal emergency requiring
expeditious diagnosis. It is important to identify Cecal volvulus on
imaging of the abdomen and pelvis in the emergency setting with
attention to the common complications that can lead to significant
morbidity in the acute phase.
References
Citation
Rao P, Kalyanpur A, Menon A. Cecal Volvulus: Retrospective Analysis of CT Evaluation in the Emergency Teleradiology Setting with a Pictorial Review of the Salient Features. Indian J Appl Radiol. 2024;10(1): 194.