Review Article
Kalgoorlie Hospital, Western Australia 1895-1897, the First Five Months of Hospital Admissions, and Typhoid in the Gold Fields
Peter Stride*
Corresponding author: Peter Stride, University of Queensland School of Medicine 23 Aland St, Wavell Heights,Brisbane, Queensland 4012, Australia; E-mail: pjostride@gmail.com
Citation: Stride P. Kalgoorlie Hospital, Western Australia 1895-1897, the First Five Months of Hospital Admissions, and Typhoid in the Gold Fields. JEnviron Soc Sci. 2015;2(2): 116.
Copyright © 2015 Stride P. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Journal of Environmental and Social Sciences | Volume: 2, Issue: 2
Submission: 15/07/2015; Accepted: 20/08/2015; Published: 26/08/2015
Abstract
Lessons from history can assist in management today by avoiding errors of the past. Kalgoorlie is a remote city in the Goldfields of Western Australia 600kms east of Perth with a current population of about 30,000. When gold was discovered there in 1893, thousands of optimistic prospectors flocked there before the development of any community infrastructure. A tent city and then a tent hospital developed, dealing with the problems inherent in remote mining communities lacking clean water and sanitation. Bars, beer and brothels traditionally arrive soon after mining strikes in Australia. Trauma, violence, typhoid and other infections including venereal diseases were common. The unusual feature is that the current Kalgoorlie Base Hospital archives records of admissions and discharges dating back to 1896. The clinical details of the first 298 inpatients admitted between 1st December 1896 and 27th April 1897 are presented.
Introduction
Kalgoorlie, now known as Kalgoorlie-Boulder after Kalgoorlieand Boulder communities joined, is a city in the Goldfields-Esperanceregion of Western Australia, Australia, located 600 kilometres eastnorth-east of Perth at the end of the Great Eastern Highway. Thename Kalgoorlie is derived from the Wangai word Karlkurla, meaning“place of the silky pears”.
In January 1893, three prospectors, Paddy Hannan, TomFlanagan, and Dan O’Shea passing through the area noticed signsof gold in the area, and stopped. By June 1893, Hannan had fileda claim, and hundreds of men swarmed to the area, some pushingwheelbarrows or riding wooden bicycles from Perth, in search of gold and the town of Kalgoorlie was born. The arrival of tens ofthousands of people before the development of infrastructure andwith unhygienic conditions, unclean water, and inadequate disposalof waste rapidly led to an epidemic of typhoid or enteric fever asit was also known. Working exposed to the Australian sun can beextremely dehydrating, and today many labourers carry ten litres ofwater per day.
The author (PS) while working in Kalgoorlie hospital experiencedtemperatures up to 47 °C, and had a 19 year old male with no previousrenal disease admitted with a creatinine over 300mmol/L in spite ofconsuming five litres of water during a day exposed to the sun inJanuary. He responded to intravenous saline with full recovery within24 h.
It was impossible over 100 years ago to find ten litres of cleanwater as workers carry today, and the prevalence of typhoid increasedin very hot spells as in 1902 when a heat wave with shade temperaturesover 100°C resulted in over 90 cases in the Kalgoorlie Hospital [1].
In 1895 a hospital opened, initially in tents, and subsequentlyin more permanent buildings. Records are available in the hospitalarchives dating back to 1896 of early admissions, two-thirds ofwhom were suffering from enteric fever caused by clinically identicalinfection with either of the water or food borne Salmonella entericaserotypes Typhi and Paratyphi.
By 1898 the town population was 2,018 (1516 males and 502females), increasing to 30,000 people in 1903, much the same as thepopulation of 31,107 at the 2011 census. The area with a populationexceeding 200,000 in the 1890s gained a notorious reputationinhabited by gamblers, bandits and prostitutes. By 1902, the townhad 8 breweries, several brothels and 93 hotels, some still functioningtoday as some of the finest examples of mining town architecture inthe world.
The mining of gold along with other metals remains a majorindustry in Kalgoorlie today, employing a quarter of Kalgoorlie’sworkforce, and generating a significant proportion of its income. Thecentral gold field area, known as the Golden Mile, is thought to bethe richest square mile on Earth. Kalgoorlie was connected by rail toPerth in 1896 and to Port Augusta in South Australia in 1917. A freshwater pipeline bringing in fresh water from Perth opened in 1903.
The History of Typhoid
The Typhoid bacillus was first detected and identified in 1880 byKarl Eberth and confirmed as the cause of the disease by Georg Gaffkyin 1884, but it is considered to have been the cause of many pastoutbreaks of infection with associated high mortality, for examplethe Athenian plague of 430BC, which killed a third of the populationincluding Pericles and the disease which wiped out the Englishsettlement of Jamestown, Virginia, USA in the early 17th century.It is thought to have caused the death of over 80,000 soldiers in theAmerican Civil War.
The association of typhoid with poor sanitation and disposal ofsewage was well known by the 1890’s. Patrick Manson in his text‘Tropical Diseases’ notes the frequency of the disease in Europeanssoon after arrival in unsanitary places in Asia, particularly fromdrinking contaminated water [2]. He writes:-‘Similar testimony hascome from Australia, where typhoid has occurred in the back countryin lonely spots, hundreds of miles from fixed human habitation ’.
William Osler was the leading global medical authority when goldwas discovered in Kalgoorlie. His text ‘The Principles and Practiceof Medicine’ describes the diagnosis and management of typhoid atthe closing of the 19th century [3]. Osler acknowledges the work ofEberth, Koch, and Gaffky in identifying the causative organism, ‘ashort, thick, motile bacillus with rounded ends which grows readily onvarious nutritive media’. He considered that ‘In cities the prevalence oftyphoid fever is directly proportionate to the inefficiency of the drainageand the water supply’. Osler noted that the mortality varied from 10-30% in different outbreaks. Improved sanitation and vaccinationintroduced late in the 19th greatly reduced mortality.
Diagnosis
Clinical features are not available from the Kalgoorlie Hospitalrecords and the accuracy of the diagnosis of typhoid is pivotal to thispaper. Osler [3] considered the presence of rose-coloured spots andsplenomegaly were key features on examination. Connor reportedrose spots in 5-30% of cases, (blanching erythematous maculopapularlesions usually 2-4 mm in diameter) usually on the abdomen andchest [4].
The history of a pre-febrile phase with headache, malaise,bronchitis and anorexia, followed by a febrile illness with diarrhoeawas strongly suggestive of typhoid. Osler considered splenic punctureto obtain a culture was rarely justified.
Management
In the pre-antibiotic era, Osler [3] believed medications were ofno avail and that careful nursing under an intelligent nurse was criticalin the management of seriously ill patients in the era also beforeintravenous fluids. He advised a low residue diet predominantly ofmilk with plenty of water, but alcohol only for weakness, high feveror a weak pulse. Patients with a high fever over 102.5oF should beimmersed in a cold bath every three hours, and severe diarrhoeawas treated with starch and opium enemata. Acetate of lead andopium were recommended for haemorrhage. Osler recognised thatneurological features, peritonism and heart failure, for which herecommended alcohol and strychnine being uncertain of the benefitsof digitalis, indicated a poor prognosis.
The Kalgoorlie Hospital and typhoid in the goldfields
There were three phases in the development of a hospital inKalgoorlie in the 1890s, a funding and planning phase, the initialtent hospital, and the finally a permanent construction with extantarchived patient records commencing about the date of opening theinitial buildings.
Planning
By 1894, the citizens of Kalgoorlie perceived a need for their ownhospital, similar to the nearby Coolgardie Hospital opened the previousyear. A meeting at the Exchange Hotel was proposed in December 1894to commence fund raising, initially with a sports event [5].
Motivated citizens with various relevant skills were gathered into acommittee to drive the construction and opening of this establishment,which would be initially under canvas. They considered that thebuilding should be constructed of stone similar to the CoolgardieHospital, and that the State Government should pay the costs as theyhad in providing hospitals for the citizens of Perth. The hospital doctorrequested that a portion of the miners subscriptions to the hospitalshould be handed over to him as extra salary, but the committeereplied they “cannot entertain his proposal [6].”
The Tent Hospital
Kalgoorlie Hospital opened in canvas tents by March 1895, withMs Alerdice as the first matron. Prior to the opening a temporarystructure known as Hannan’s hospital received a few patients [7].
In September a miners’ public clinic between 1000 and 1100 hours and again between 1900 and 2000 hours was commenced. Thecommittee requested a district sanitary inspector and an improvedwater supply from the Government to reduce water-borne diseasesamong the rapidly increasing population.
Fortnightly fund raising smoke concert were organised, and thepositions of hospital medical officer with private practice for £200 perannum, and of a matron, for £151 per annum with free quarters wereadvertised [8].
In an era before mass production of cigarettes and the obviousadverse effect of tobacco, the hospital doctor, Dr. O’Mahon, presidedover a well-attended concert and smoke social in Waldack’s Club toraise funds for the Kalgoorlie Hospital [9].
Miss Bessie Way, daughter of Dr. E. W. Way, honorary surgeonand board member of the Adelaide Hospital, and niece of the deputyGovernor of South Australia Chief Justice Way, successfully appliedfor the position of matron. She was described as a highly accomplishednurse following the best possible training at the Adelaide Hospital[10,11].
Little information about typhoid in the Kalgoorlie district isavailable before 1896, but Dr Barber reported three deaths fromtyphoid in six months between August 1895 and February 1896,and then a slight increase in the mild cases of typhoid admitted tothe Kalgoorlie hospital in January. With unfortunate and erroneousoptimism saw no reason to anticipate any serious outbreak of typhoidin the district [12].
In February 1896, the tent hospital had 24 beds. The hospitalorganisation was criticised in the local paper when four patients wererefused admission due to the lack of available beds, in spite of theapparent availability of four other large tents which could have beenerected immediately [13]. In March 1896 the Works Departmentaccepted a tender to erect hospital tents containing thirty extra beds.The tents were made of navy canvas erected under a single iron roofto shelter nursing staff passing from ward to ward [14].
In March 1896, a Mr Geoghegan complained to the localnewspaper about a gentleman refused hospital admission withoutmedical review in spite of severe pain. Dr J.A. O’Meehan, the R.M.O.defended his patient care by responding that the complaint wassomewhat exaggerated as the patient had a boil on his leg requiringoutpatient treatment. O’Meehan stated that the hospital was openfor public inspection on specified afternoons, an idea which couldbe adopted today [15]. Enteric fever became more prevalent duringFebruary when Dr. O’Meehan reported 24 admissions suffering fromtyphoid with one death, amongst a total of 41 admissions with fivedeaths [16].
Bishop Gibney stated that the new St. John of God KalgoorlieHospital building would be open at all hours of the day and nightfor urgent admissions regardless of creed and that clergyman of alldenominations would have free access to their parishioners [17].Clergymen were not immune from illness and the Rev A. J. Burt wasreported to be improving in December 1986 after a long admission[18], and similarly, Father Deasy was approaching discharge in April1897 also after a long illness in the Kalgoorlie Hospital [19].
By April 1896, Kalgoorlie Hospital had 56 beds, with proposalsfor another 34. The risk to hospital staff of catching diseases wasdemonstrated in April 1896, when both Dr. O’Meehan, the hospitalmedical officer, and Miss Bessie Way, the matron, contractedtyphoid. Clearly the position of matron was not an office job then.Dr. O’Meehan recovered uneventfully and was expected to returnto work shortly, while Dr. Barber worked as locum medical officer.Bessie Way was not admitted suggesting a mild attack. She returned toher home in Adelaide by coach to Albany, then steamer to Adelaide,for a month’s convalescence accompanied by her mother, who hadnursed in her daughter’s place and ‘moved about in the sick wards likea ministering angel’.
The typhoid epidemic worsened in April. 64 of the 76 patientsadmitted had typhoid, which caused five of the seven deaths. TheColonial Secretary approved Dr. J Barber’s telegram request foranother ward, but it was not erected as the outbreak subsided for awhile [20,21]. Soon after Bessie Way’s return, she became engaged toMr. Harvey, of Kalgoorlie, which then necessitating her retirementfrom nursing, and Miss C. H. Bucklay was appointed as matron of theKalgoorlie Hospital [22,23].
In spite of cooler weather, typhoid caused 96 of the 113 admissionsplus four of the six deaths in June 1896, and 18 of the 36 admissions,plus seven of the eight deaths in July in Kalgoorlie Hospital [23,24].By October, plans for the new hospital were well advanced and Dr.O’Meehan visited Perth for a few days to give an expert medicalopinion, then considered important in the construction of a newhospital [25].
Records, currently archived in the Kalgoorlie Hospital, ofadmissions to the Hospital date from December 1st 1896. This paperreviews the first 298 patients admitted between that date and April27th 1897, with the last of the being discharged on 3rd September 1897after 101 days in hospital. The tent hospital had been open at leastsince late 1895 and some details are available in local papers, the morepermanent structure was opened about February 1897, though thedate is not clear.
The Permanent Building
Construction of the St. John of God’s Hospital building to replacethe tent hospital commenced in late 1896, and by January 1897 hadprogressed sufficiently to anticipate the admission of patients withinthree weeks. The paper reported ‘The front set of rooms, comprisingthe sisters’ quarter’s, a reception-room, the kitchen and the scullery,the washhouse, &c., is rapidly approaching the final stage. The sisters’rooms are thoroughly ventilated in the walls and ceilings. They havefire places, and are painted and papered in a. refreshing tint, with adado of fluted iron, a wooden skirting, and a bordering of wood. Theceiling is of fluted iron also. The building alone will cost about £3,800,and the framing will need an expenditure of between £40 and £500’[26].
Three miners’ deaths in the Kalgoorlie Hospital were reportedin February and recorded in the admissions and discharges. One ofthem Michael O’Grady, was admitted with typhoid on 22/1/1897 anddied six day later [27].
The co-located Mrs. Mecham’s Kalgoorlie Private Hospital, wasfirst mentioned when destroyed by fire! The fire broke out in a bushshed an evening in March about 7 o’clock where one of the nurseswas lighting a lamp, unfortunately igniting the shed. The fire thenadvanced too rapidly to prevent its progress. The eighteen patients inthe building at the time, all suffering from typhoid, were all evacuatedand safely transferred to the Government Hospital. The onlysignificant injury was to the recently arrived police constable Baxter’sspine through a fall over a log of wood, and he was also conveyed tothe Hospital [28].
The new Kalgoorlie Hospital was visited by the state Premier, whowas subsequently farewelled with hearty cheers at the railway station,presumably for his attendance, rather than his departure [29,30]. TheDispensers J. Boilean & Co were awarded the pharmacy position inthe new hospital building.
The current Perth based principal medical office, Dr. Lovegrove,paid an official visit to Kalgoorlie hospital in July 1897. Dr Lovegrovesupported the hospital doctor in public health issues [31]. In August1897, Miss Lee, previously matron of the Coolgardie Hospital, becamematron of the Kalgoorlie Hospital [32].
Between December 1st, 1896 and April 27th 1897, 195 out of298 (65%) admissions to Kalgoorlie Hospital had typhoid with 34deaths (mortality rate 17%). 38% of these cases were miners, and 15were involved in the preparation or distribution of food and drink,as storekeeper (2), butcher (2), baker (2), house keeper, brewer,hotel servant, cellarman, barman, brewer, housemaid, cordialmanufacturer and domestic, and therefore a serious risk factor in thedissemination of the disease. 18 other patients were admitted with thediagnosis of diarrhoea, dysentery and peritonitis, some of whom mayalso have had typhoid. Two patients with typhoid were suspected ofhaving intestinal perforation, both died. The only nurse admitted toKalgoorlie hospital in the study period was Emily Herbert, aged 25,with influenza for 12 days followed by uneventful discharge.
After the initial typhoid epidemics swept the goldfields nosubsequent epidemic disease had such a serious impact. Othercommon infections at the time included influenza, bronchitis,tuberculosis and meningitis, and there were also many admissionswith trauma sustained in the mines and elsewhere.
Fresh water and Charles O’Connor
Kalgoorlie finally obtained a fresh water supply, pumped fromPerth thanks to the vision and engineering expertise of an IrishmanCharles O’Connor. He became Engineer-in-Chief of WesternAustralia in 1891. He is best known for the construction of Freemantleharbour, but the construction of a pipeline from Mundaring Weirnear Perth was a unique feat in engineering at that time. Forrest thepremier approved a loan of £2.5 million. 5 million imperial gallonswas pumped in eight successive stages through 530 km of 760 mmdiameter pipe to Kalgoorlie. Unfortunately O’Connor was criticisedin parliament and the media as incompetent and corrupt, resultingin his suicide a month before the pipe commenced sending water toKalgoorlie. A subsequent inquiry belatedly cleared him of any wrongdoing. O’Connor, an expert professional, was politically naive andunaccustomed to the mud-slinging of politicians. Today his visionand skill are recognised and an electorate in Western Australia isnamed after him [33] (Table 1).
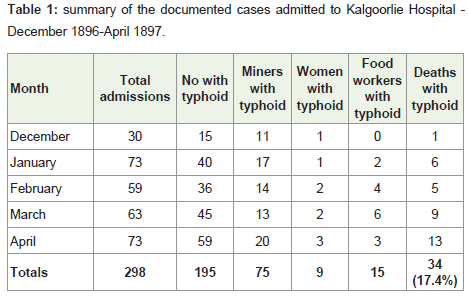
Table 1: Summary of the documented cases admitted to Kalgoorlie Hospital -December 1896-April 1897.
Kalgoorlie Hospital today
Kalgoorlie Hospital, the largest regional public hospital in WesternAustralia is a 131-bed inpatient facility, with a 24 h EmergencyDepartment servicing over 20,000 patients per year, a coronary care/high dependency unit, a dialysis unit plus medical, surgical, obstetricsand gynaecology, paediatric, mental health, and orthopaedic wards.Sub-specialists in ENT, Urology, Ophthalmology and Oncology visitregularly and the Royal Flying Doctor is available to take complexand critical cases to tertiary hospitals in Perth. Trauma from motorvehicle accidents and mining injuries and alcoholism are common.
Past terminology
Some terms appear in the ‘designation’ or diagnostic columnthat are no longer in common usage. Morbus cordis means heartdisease, possibly heart failure, but usually used when a more specificdiagnosis is not clear; phthisis specifically meaning wasting, butused almost specifically for tuberculosis: cholera nostras is an illnesssimilar to cholera: ptomaine poisoning means food poisoning by amicroorganism, simple continuous fever means exactly that, a nonspecificterm still found in homeopathy texts, and capillary bronchitisis now termed bronchiolitis.
Typhoid in the 21st century
Typhoid, or enteric fever, remains a severe global problemcompounded by increasing antibiotic resistance, limited vaccineefficacy and international tourism today with an estimated 22 millioncases annually and an estimated 200,000 - 600,000 deaths [34]. In thetwenty-first century enteric fever has largely become a disease of thethird world where standards of water cleanliness and sanitation aresuboptimal. It is found mainly in Asia where an estimated 13 millioncases occur annually, with 400 000 deaths, particularly following waror natural disasters where water supplies become polluted. Childrenhave disproportionately increased levels of morbidity and mortality.
Chloramphenicol, Ampicillin, and Co-trimoxazole have beenused to treat typhoid since they first became available, howeverChloramphenicol resistance had become widespread forty years ago,and resistance to all three has been detected in Asia for over twenty years. Flouroquinalones have become the drug of choice. Currentvaccines are ineffective against S. paratyphi, the predominant tourists’pathogen, and provide only moderate protection against S. Typhi [4].
In first world counties, typhoid has become a disease of youngunvaccinated tourists to Asia. Improvements in sanitation andhygiene between 1920 and 1990 reduced the annual number of casesin USA from about 36.000 to approximately 500. The proportionacquired during foreign travel over the thirty years between 1967 and1997 has increased from 33% to 81% [4].
Lynch reported 1902 typhoid fever cases, median age 22 years,detected in USA between 1999 and 2006, 1295 (73%) requiredhospitalization and 3 (0.2%) died. 1439 (79%) reported foreigntravel in the previous 30 days of illness, only 58 travellers (5%) hadbeen vaccinated against typhoid. 272 (13%) of 2016 isolates testedwere resistant to ampicillin, chloramphenicol, and co-trimoxazole(multidrug-resistant S Typhi) [35].
Enteric fever still occurs in Australasia. Auckland Hospitalreported 162 confirmed cases in a six year period, 50% havingtravelled beyond the Pacific area, 25% had travelled within the Pacificand 25% had not left New Zealand. 83% were Salmonella typhi. Feverand diaphoresis were reported by 91% of patients, but only 61% haddiarrhoea. Ciprofloxacin and amoxicillin were the most commonlyprescribed antibiotics. The median length of stay was six dayscompared with 50 days a hundred years ago and there were no deathscompared with 17% in the gold rush days of Kalgoorlie. However 28%of the New Zealand cases had a recent previous admission to hospitalwith probable typhoid when the correct diagnosis was not made,probably a higher figure than in early Kalgoorlie where familiaritywould generate a higher level of suspicion.
Conclusion
Enteric fever caused most of the admissions and deaths inthe Kalgoorlie hospital in the early days of the gold rush 120 yearsago. In spite of the advances since then, the disease remains a verycommon cause of essentially preventable morbidity and mortality ina world where first world greed and labels appear more importantthan providing a safe supply of water in the third world. The thirdworld needs a Charles O’Connor! The problem will be increasinglyexacerbated by progressive antibiotic resistance and the limitedefficacy of current vaccines unless we act soon to ensure safe waterall over the world.
References
- (1902) Sunday Times Perth, Sunday 20th April.
- Manson P (1898) Tropical Diseases. Cassell and Co London 193-196.
- Osler W (1892) The Principles and Practice of Medicine. Appleton and Co New York 1-39 D.
- Connor BA, Schwartz E (2005) Typhoid and paratyphoid fever in travellers. Lancet Infect Dis 5: 623-628.
- (1894) Western Argus, Saturday 15th December.
- (1895) Western Argus, Thursday 29th August.
- (1894) Western Argus, Saturday 22nd December.
- (1895) Western Argus, Thursday 12th September.
- (1895) Kalgoorlie Miner, Saturday 28th September.
- (1895) Kalgoorlie Miner, Monday 30th September.
- (1895) The West Australian, Friday 4th October.
- (1896) The Daily News Perth, Wednesday 12th February.
- (1896) Kalgoorlie Western Argus, Thursday 27th February.
- (1896) The Daily News Perth, Tuesday 3rd March.
- (1896) Kalgoorlie Miner, Wednesday 25th March.
- (1896) The Inquirer and Commercial News Perth, Friday 27th March.
- (1896) The Inquirer and Commercial News Perth, Friday 17th April.
- (1896) Kalgoorlie Miner, Saturday 19th December.
- (1897) The Daily News Perth, Monday 12th April.
- (1896) The Inquirer and Commercial News Perth, Friday 1st May.
- (1896) Kalgoorlie Western Argus, Thursday 6th August.
- (1896) The Inquirer and Commercial, News Perth Friday 10th July.
- (1896) The Daily News Perth, Friday 7th August.
- (1896) Kalgoorlie Miner, Saturday 3rd October.
- (1897) Kalgoorlie Western Argus, Thursday 28th January.
- (1897) Kalgoorlie Western Argus Thursday 4th February.
- (1897) Western Mail Perth, Friday 12th March.
- (1897) The West Australian Perth, Monday 3rd May.
- (1897) The West Australian Perth, Friday 9th July.
- (1897) The West Australian Perth, Thursday 22nd July.
- (1897) The Daily News Perth, Tuesday 27th July.
- Merab Harris Tauman (1988) O'Connor, Charles Yelverton (1843-1902) Australian Dictionary of Biography, National Centre of Biography, Australian National University, yelverton-7874/text13685, published first in hardcopy 1988, accessed online 16 July 2015.
- Bhutta ZA, Threlfall J (2009) Addressing the global disease burden of typhoid fever. JAMA 302: 898-899.
- Lynch M, Blanton E, Bulens S, Polyak C, Vojdani J, et al. (2009) Typhoid Fever in the United States, 1999-2006. JAMA 302: 859-865.
- Lane RJ, Holland D, McBride S, Perera S, Zeng I, et al. (2015) Enteric fever in the Pacific: a regional retrospective study from Auckland, New Zealand. Intern Med J 45: 148-155.