Research Article
Weight Gain Pattern During Pregnancy amongWomen Attending for Normal Labor at Makasar Primary Health Care, Jakarta
Muhammad Yusra Firdaus1*, Biyan Ramadhan1, Muhammad Iqbal Maulana1, Nabella Qisthina Laksita Dewi1, Nur Mentari Sofyan Putri1, Ikhwanuliman Putera1, Aliefatin2 and Herbert Situmorang2
1Faculty of Medicine, University of Indonesia, Jakarta, Indonesia
22Department of Obstetric and Gynaecology, Faculty of Medicine, University of Indonesia - Cipto Mangunkusumo Hospital, Jakarta, Indonesia
Corresponding author: Muhammad Yusra Firdaus, Faculty of Medicine, University of Indonesia, Jakarta, Indonesia, Telp:+628567934763; E-mail: yusrafirdaus@rocketmail.com
Citation: Firdaus MY, Ramadhan B, Maulana MI, Dewi NQL, Putri NMS, et al . Weight Gain Pattern During Pregnancy among Women Attending for Normal Labor at Makasar Primary Health Care, Jakarta. Indian J Nutri. 2015;2(1): 113.
Copyright © 2015 Muhammad Yusra Firdaus, et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Indian Journal of Nutrition | ISSN: 2395-2326 | Volume: 2, Issue: 2
Submission: 18/10/2015; Accepted: 02/11/2015; Published: 07/11/2015
Abstract
Background: Maternal nutritional stutus before and during pregnancy were important for optimal pregnancy outcomes. Institute of Medicine had alreadypublished guideline for proper weight gain during pregnancy. Women in Jakarta, a metropolitan area of Indonesia,are in relatively younger age of marriage.Previously, its was reported that maternal nutritional stutus among young mother was poor. Thus, this study aimed to know the pattern of weight gain amongpregnant women in Jakarta setting.
Methods: This study was a retrospective study using medical records ofpregnant women undergone normal labor in Makasar Primary Health Care,Jakarta during 2014. The data included in this study are pre-pregnancy weight, body mass index, and weight gain during pregnancy. Institute of Medicinerecommendation was used to classify maternal body weight gain.
Results: A total of 128 medical records were included in this study. We found that the majority of pregnant women had poor weight gain (71 subjects,55.5%) compared to ideal weight gain (39 subjects, 30.4%) and excessive weight gain (18 subjects, 14.1%). Most subjects in underweight and normoweightwomen had poor weight gain compared to overweight and obese women (p< 0,001). Body mass index before pregnancy was correlated with body weight gain(r= -0.374, p<0,001).
Conclussion: Most of women attending fornormal labor in Makasar Primary Health Carehad poor weight gain during pregnancy.
Keywords: Body mass index; Normal labor; Pregnancy; Primary health care; Weight gain
Introduction
Nutritional status before and during pregnancy are considered important for optimal pregnancy outcomes regarding optimalnewborn birthweight and maternal body weight after pregnancy [1].Previous study showed that excessive weight gain during pregnancywas associated with increased risk of maternal hypertensionduring pregnancy, gestational diabetes, caesarean delivery, preeclamsia, haemorrhagic post-partum events, macrosomia,neonatal hypoglicemia, and even intrauterine fetal death [1,2].However, inadequate maternal weight gain during pregnancy wasalso detrimental for the newborn as it would increase the risk ofhaving low birth weight newborn, prematurity, problems relatedto infant’s growth and development, and risk of physical disabilitylater in lifetime. To date, Institute of Medicine (IOM) had publishedrecommendation for optimal maternal weight gain during pregnancy based on maternal body mass index (BMI) before pregnancy [1].
From Indonesia Demographic and Health Survey 2012, it wasshown that the median age at first marriage among Indonesianreproductive women was quite younger, 20.4 years old [3]. Shirimaet al. showed that maternal nutritional status among younger motherwas poor. Also, younger mother tend to be anemic and thus correlatedwith newborn birth weight [4]. Therefore, we performed studyin Jakarta population to know maternal nutritional status duringpregnancy reflected by weight gain. Knowing maternal nutritionalstatus among pregnant women and associated factors in this settingwould be beneficial for further intervention in high risk population.
Materials and Methods
Study desain
This was a retrospective study using medical records of pregnantwomen undergone normal labor at Makasar Primary Health Care,Jakarta from January to December 2014. Medical records werecollected consecutively. Inclusion criteria were mothers with normallabor (no complication, full term baby >37 weeks of gestation age,and performed vaginal delivery). Samples with severe preeclampsia,stillbirth, or without antenatal care records were excluded. Also,medical records with incomplete data of weight before, at the endof first trimester, at the end of second trimester, and before deliverywere excluded.
Data collection
The data collected from medical records included characteristics(age and level of education), frequency of antenatal care (ANC) visit,gestational week for the first ANC visit, haemoglobin (Hb) level atfirst trimester, and serial body weight during routine follow-up ofANC visits. Weight before pregnancy data were noted in medicalrecord based on interview to the mother while serial measurementswere noted from weighing directly. Tolerance up to two weeks wasused in determining trimester, otherwise the data were not counted.BMI were then calculated using modification for Asian populationproposed by World Health Organization [5]. IOM recommendationwas adopted to estimate ideal body weight gain for pregnant women.Underweight women (BMI< 18.5 kg/m2 is ideally gain 12.7-18.1 kgduring pregnancy, normal weight women 11.3-15.9 kg, overweightwomen 6.8-11.3 kg, and obese women5.0-9.0 kg [1]. Maternal agewere also classified regarding risks of pregnancy outcomes withmaternal age 20-34 considered to have lesser risk [6]. Mother wereconsidered anemic if Hb level for the first trimester was below 11 g/dl [7].
Statistical analysis
Statistical analysis were done using SPSS 16 (Statistical Packagefor Social Science, Chicago, Inc.) for windows. Numeric data weretest for normality of the distribution using Kolmogorov-smirnovtest. Normally distributed data were presented as mean ± standarddeviation while non-normally distributed data were presented asmedian (minimum-maximum). Chi-square test was used to findassociation between category of BMI and category of weight gain.All correlation were also tested using either Pearson or Spearmancorrelation tests if the data were normally or non-normally distributed, respectively. P value <0.05 was considered significant.
Results
A total of 128 pregnant women were included in this study as theyfulfilled the inclusion and exclusion criteria. As many as 110 subjects(85.9%) were in 20-34 age group. Most of subjects (126 subjects,98.4%) had minimally four ANC visits at Makasar Primary HealthCare. Mean BMI of subjects was 22.9 ± 4.3 kg/m2. Characteristics ofsubjects including maternal BMI and adequacy of weight gain werepresented in Table 1.
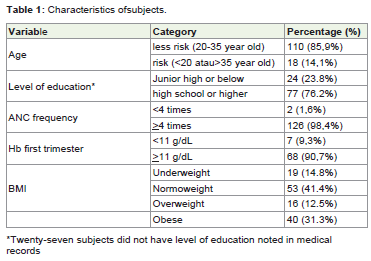
Table 1: Characteristics of subjects.
Median weight gain during pregnancy was 9,0 kg (-11.0- 25 kg). Three subjects lose weight during pregnancy. UsingIOM recommendation, more than half of subjects failed to gainrecommended weight (71 subjects, 55.5%). Underweight andnormoweight women tend to had poor weight gain during pregnancycompared to overweight and obese women (p< 0,001, Table 2). Weightgain was correlated with BMI before pregnancy (r= -0.374, p< 0,001).Level of education, age at higher risk, anemic status, frequency ofANC visit did not assocaited with weight gain category (p>0.05).
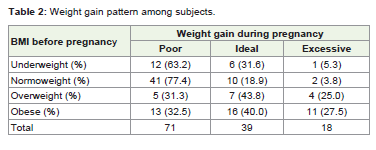
Table 2: Weight gain pattern among subjects.
Discussion
The main finding of this study was although nearly all subjects hadminimal of four ANC visits, majority of pregnant women in Jakarta,metropolitan area of Indonesia, failed to achieve recommendedbody weight gain during pregnancy. We also found that BMI beforepregnancy had significant correlation with weight gain.
Our study was perfomed in developing country with more thanfive percent baby born as low bith weight baby [3]. In contrast toour finding, Deputy et al. performed a study in America and foundthat majority of women increase weight gain in excessive manner (47.2%). They also found that many factors including race, level ofeducation, and also BMI before pregnancy associated with weightgain in that population [8]. Another study in America found that43.7% population were categorized as having excessive weight gainand only 22% considered as poor weight gain. Interestingly, theyfound thatmajority of pregnant women with excessive weight gainwere obese before pregnancy [9].
Our result also similar to Winkvist et al. study. They found thatin rural area in Purworejo, Centra Java, BMI before pregnant, levelof education, and level of socio-economic status was associated withpoor weight gain during pregnancy [10]. We proposed that differentpopulations have different habbit, pattern of eating, faith aboutprohibition of food during pregnancy and food supply in specific area[10], however, most of rural and metropolitan population also failedto gain recommended weight gain.
The importance of maternal weight gain should be emphasizedbyphysician facing pregnant women. Indonesia is currently shiftedtoward implementation of universal health coverage with fullimplementation in 2019. Thus, primary health care is fundamentalto deliver good health care, including toward pregnant women.Monitoring maternal weight gain during pregnancy plays pivotalrole as it correlated with newborn birth weight [11,12]. In this study,although pregnant women fulfilled minimum of four ANC visit, theystill could not met recommendation. Therefore, physician in primaryhealth care should addressed this problem so that mother could hadoptimal weight gain and hopefully would deliver optimal infant.Primary health care as a frontier of health system had a responsibleto prepare mother prior pregnancy especially their nutritional status.From previous study, BMI was associated with population knowledgeregarding optimal food serving size [13]. In Jakarta setting, physicianmight not only rely on mother’s level of education. Also, maternalpreparation including good nutrition before pregnancy is important.
This study had several limitations. Firstly, This study onlyconducted in a single primary health care in Jakarta. Given the totalnumber of PHC in district level, the generalization to other settingis limited. This result, however, still beneficial for other communitysettings which have comparable characteristics. Secondly, we couldnot addressed the nutritional intake status among subjects as weonly measured outcomes of nutritional mainly BMI. The weightbefore pregnancy data were based on interview to the mother thusit might be under- or overestimate from the exact ones. This wasdue to lack of medical data record because visiting physician was notroutinely done by most Indonesian people. We also lack informationof macronutrient and micronutrient status. Maternal perception andknowledge of food and nutrition were also not analyzed.
Conclusion
This study found that majority of pregnant women in Jakarta,metropolitan area of Indonesia, failed to gain recommended weightgain during pregnancy. Maternal BMI before pregnancy wascorrelated with body weight gain during pregnancy.
Acknowledgement
We thank to Makasar Primary Health Care staff who cooperatedin this study.
References
- American College of Obstetricians and Gynecologists (2013) ACOG Comittee opinion. 548: weight gain during pregnancy. Obstet Gynecol 121: 210-2.
- Li N, Liu E, Guo J, Pan L, Li B, et al. (2013) Maternal prepregnancy body mass index and gestational weight gain on pregnancy outcomes. PLOS ONE 8: e82310.
- Statistics Indonesia (Badan Pusat Statistik—BPS), National Population and Family Planning Board (BKKBN), and Kementerian Kesehatan (Kemenkes—MOH), and ICF International (2013) Indonesia Demographic and Health Survey 2012. Jakarta, Indonesia: BPS, BKKBN, Kemenkes, and ICF International.
- Shirima CP, Kinabo JL (2005) Nutritional status and birth outcomes of adolescent pregnant girls in Morogoro, Coast, and Dar es Salaam regions, Tanzania. Nutrition 2: 32-38.
- WHO Expert Consultation (2004) Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet 363: 157-163.
- Laopaiboon M, Lumbiganon P, Intarut N, Mori R, Ganchimeg T, et al. (2014) Advanced maternal age and pregnancy outcomes: a multicountry assessment. BJOG 121(Suppl 1): 49-56.
- Centers for Disease Control CDC (1989) criteria for anemia in children and childbearing-aged women. MMWR Morb Mortal Wkly Rep 38: 400-4.
- Deputy NP, Sharma AJ, Kim SY, Hinkle SN (2015) Prevalence and characteristics associated with gestational weight gain adequancy. Obstet Gynecol 125: 773-781.
- Schieve LA, Cogswell ME, Scanlon KS (1998) Trends in pregnancy weight gain within and outside ranges recommended by the institue of medicine in a wic population. Matern Child Health J 2: 111-116.
- Winkvist A, Stenlund H, Hakimi M, Nurdiati DS, Dibley MJ (2002) Weight-gain patterns from prepregnancy untul delivery among women in Central Java, Indonesia. Am J Clin Nutr75: 1072-1077.
- Muthayya S (2009) Maternal nutrition & low birth weight - what is really important? Indian J Med Res 130: 600-8.
- Abrams B, Selvin S (1995) Maternal weight gain pattern and birth weight. Obstet Gynecol 86 : 163-169.
- Shah M, Adams-Huet B, Elston E, Carson K (2010) Food serving size knowledge in African American women and the relationship with body mass index. J Nutr Educ Behav 42: 99-105.