Review Article
Effect of Protein Energy Malnutrition on the Diarrheal Electrolyte Imbalance in Children of Chittagong Region, Bangladesh
M F Quamar* and S K Bera
Corresponding author: Md. Atiar Rahman PhD, Associate Professor, Department of Biochemistry and Molecular Biology, University of Chittagong, Chittagong-4331, Bangladesh, Tel: +88-031-2606001-10, Ex-4334, Cell: 01711709084, Fax: +88-031-2606014,; E-mail: atiarh@yahoo.com
Citation: Akhter S, Alauddin M, Rahman MA, Chowdhury MA. Effect of Protein Energy Malnutrition on the Diarrheal Electrolyte Imbalance in Children of Chittagong Region, Bangladesh. Indian J Nutri. 2014;1(1): 101.
Copyright © 2014 Md. Atiar Rahman et al. This is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Indian Journal of Nutrition | Volume: 1, Issue: 1
Submission: 24/04/2014; Accepted: 17/06/2014; Published: 20/06/2014
Reviewed & Approved by Dr. Idrees Ahmed Wani, Assistant Professor, Department of Food Scienceand Technology, University of Kashmir, India
Abstract
The study was carried out to identify the risk factors involved in the development of Protein Energy Malnutrition and its effect on the diarrheal electrolyteimbalance in Bangladeshi children. Among a 100 protein energy malnourished children, 64 ±1.02% patients (Group-A) were edematous with 39 ± 0.93%kwashiorkor and 25 ± 0.78% marasmic kwashiorkor whereas 36 ± 0.86% (Group-B) was marasmic with 39 ± 0.77% diarrhea. Thus the patients have beensuffering from acute respiratory infection 25 ± 0.35%, septicemia 29 ± 0.66%, tuberculosis 7 ± 0.36% and other secondary infections. Analysis of serumelectrolytes revealed that hypokalemia was seen in 46 ± 0.84% patients of Group-A and 20 ± 1.01% of group B. Hypernatremia (Group-A) was seen in 14 ±0.64% patients, low serum in 52 ± 0.55% while 32 ± 0.73% of them had diarrhea. Serum total protein and albumin of the kwashiorkor group were significantly(p< 0.01) higher (39 ± 0.65%) than marasmic (36 ± 0.99%) and Marasmus Kwashiorkor (25 ± 0.45%) patients. The results demonstrate that protein energymalnutrition significantly affecting electrolytes of diarrheal children in Chittagong.
Keywords: Marasmus; Hypokalemia; Hypernatremia; Diarrhea; Total protein
Introduction
Malnutrition is a major global problem [1] which interacts with diarrhea in a vicious cycle leading to high morbidity and mortality in children and it is as well as a complicating factor for other illness in developing countries. Malnourished children have long lasting, severe and recurrent diarrhea. The prevalence of diarrhea is 5-7 times more in malnourished as compared to normal children [2]. In malnutrition various abnormalities occur in body electrolytes which become more pronounced with diarrheal incidence since electrolytes conduct an electrical current, helps to balance pH and facilitate thepassage of fluid between and within cells through process of osmosis imparting in regulation of the function of neuromuscular, endocrine and excretory systems [3,4].
The term protein energy malnutrition (PEM) refers to a class of clinical conditions that may be caused by energy (calorie) inadequacy [5,6]. Deficiency of proteins is usually not primary and isolated. Almost always it appears to be due to poor intake of food as such. Among the various factors that influence the clinical manifestationsof PEM, magnitude of deprivation, its duration, relative inadequacy of different principles of food and the accompanying infection or some other diseases are noted well. Two major clinical syndromes kwashiorkor and nutritional marasmus are also widely recognized. There is a definite association between malnutrition and theseinfections [7].
PEM is one of the most common immunodeficiency problems, in pediatric practice, which breaks down the host resistance largely in all segments [8]. The most consistent abnormality detected in various studies has been the impairment in cell-mediated immunity (CMI) that explains the cause of bacterial infections and type of CMI for host’s defense against them is very severe in children suffering from PEM. Kwashiorkor is the edematous form of protein energy malnutrition. It is associated with extreme poverty in developing countries and with chronic mal-absorptive conditions such as cysticfibrosis in developed countries [9,10].
PEM-caused diarrhea still constitutes another leading cause of morbidity and mortality. Almost over 500 million children suffer from acute diarrhea annually of them 5 million die every year [11]. It is said that the concentrations of individual ion influence the properties and behavior of excitable membrane such as nerve cell and performance of many intracellular enzymes are involved in such diarrheal causation. Studies showed the association of malnutrition with increased incidence and duration of acute diarrhea [12]. In severe malnutrition significant risk factor for fatal diarrhea includes hypokalemia and metabolic acidosis as intracellular Na+ retention occurs in PEM. Intracellular increase in Na+ and decrease in K+ may adversely affect the function of important enzymes of carbohydrate metabolism and oxidative phosphorylation [13].
Regulation of Na+/K+ depends upon excretion, intake, absorption occurs through gastro intestinal system. Disorders of Na+/K+ homeostasis can occur due to excessive loss, gain or retention of the Na+/K+ or H2O. A vigorous imbalance of these two ions causes hyponatremia/hypokalemia and hypernatremia/hypokalemia. Remarkably, hypokalemia and hyponatremia are seen more frequently in diarrheal population than non-diarrheal.
Chittagong is the biggest port city of Bangladesh getting a lot of PEM caused diarrheal children in rural and slum area. Significant numbers of children are suffering from acute and chronic diarrhea every year but no study has been conducted to explore the nature andcause of such diarrhea. This study has been designed to investigate the effect of protein energy malnutrition in electrolyte status in causing diarrhea to the children of Chittagong region.
Materials and Methods
This study was carried out during the period commencing on 2nd March, 2009 in nutrition block, Department of pediatrics in Chattagram Maa-Shishu O General Hospital (CMOSGH) and completed on 30th November, 2009, over one hundred children (age limit; 6 month to 5 Year) were selected who fulfilled the diagnostic criteria for PEM of WHO. This is a descriptive study where childrenwere divided into 2 groups,
Group A: 39% children who had diarrhea
Group B: 61% children who did not have diarrhea.
They were matched according to age, sex, height, weight and mid-upper arm circumference (MUAC) of the children. Each group was again divided into 2 subgroups according to presence or absence of edema. This prospective study involved children admitted to CMOSGH. The mother or guardians were informed of the purpose of the study. For each patient a detailed history was taken from motheror the attendant and recorded in a data collection sheet and through clinical examination at admission and daily follow up was recorded during the hospital stay. Children those fulfilled the inclusion criteria were included for this study.
Blood Sample analysis
A 2 ml of blood was collected from superficial vein of each child. The blood sample was taken to the laboratory for serum electrolytes estimation. Serum was separated by centrifuging (at room temperature) the blood at 3000 rpm. Total serum electrolytes(Na+, K+, Cl+, HCO3-, Hb, TC, DC) were estimated in the Biochemistry laboratory of CMOSGH. On the basis of clinical suspicion as causal factors of hypokalemia, hyponatremia, hypernatremia, the venous blood was investigated in the clinical pathology of CMOSGH forComplete blood count, differential count. Electrolytes status was measured in the department of Biochemistry, CMOSGH. Serum status was measured by using auto-analyzer (Humalyzer 2000, Human, Germany). Prepared questionnaire and history sheet was filled up for each subject. A structured questionnaire was developed and revised after pre testing for the survey. The questionnaire comprises 5 parts. The whole procedure was conducted with theconcern of the departmental ethical committee.
Part A: Included the formation of name father’s name, mother’s name, age, sex, socioeconomic status and area of living of the patients.
Part B: Included anthropometrical measurements (heightweight, MUAC). In taking height and weight in the same vertical line alongside a graduated wooden scale fixed to a wall and looking straight ahead in the same horizontal line at an object fixed to the opposite wall. Weight was measured by spring balance.
Part C: Included at the state of vaccination, present or absent of edema, diarrhea, pattern of feeding, time of weaning, eye signs, and presence or absence of dermatitis.
Part D: Included biochemical measurements, as serum electrolytes (Na+, K+, HCO3-, Cl-)
Part E: Included routine examination of blood TC and DC (Neutrophil, Lymphocytes, Eosinophil, Monocytes) and status of Hb were accomplished by the technicians, according to WHO criteria and the date were collected. Data presentation and statistical analysis
Data and results were presented in the form of figures. Collected data was checked for its completeness, correctness. Editing was done and then data were entered into computer. Analysis was done by employing Statistical Package for Social Science (SPSS Version 12.0) software package. Data were expressed as means± SD, number ofpatients and percentage of patients. To compare mean values was done as appropriate. P< 0.05 was considered as minimum level of significance.
Results
Analysis of serum electrolyte in both the groups revealed that hypokalemia, hypernatremia and low serum bicarbonate were seen more frequently in patients who had diarrhea (Group A=39) compared to who hadn’t (Group B=61). In Group-A, hypokalemia was seen in 46% patients while it was observed in 20% patients inGroup-B. Hypernatremia (Group-A) was seen in 14% patients,52% patients had low serum while 32% of them had diarrhea levels with serum total protein and albumin of the kwashiorkor group were significantly higher (39%) than marasmic patients (36%) and marasmus kwashiorkor patients (25%). Serum electrolytes analysis revealed the status of the patients with hypo and hyper electrolytic conditions (Figure 1).
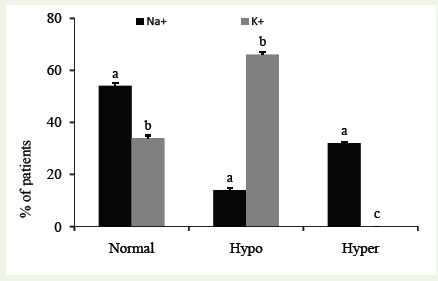
Figure 1: Serum electrolyte status in PEM children. Data are shown asmean ± SD for triplicate of each group. a&b superscript letters shown on the bar graph indicate that the values are significantly different (Tukey multiple range, post hoc test, p< 0. 05) from each other (**p< 0.01, SPSS for windows, version 18.0).
Criteria analysis showed that 90% of the children (patients) were from lower classes while 8% from middle classes and 2% from upper classes. Their feeding status pointed that 85% of the children are associated with mal-feeding while 8% were full-quenched breastfeeding and others were dependent on artificial (2%) as well as mixed (5%) feeding. Patients distribution showed that almost 80% of the children were 50-75 cm, 18% were 70-100cm and only 2% children were >100 cm (Figure 2).
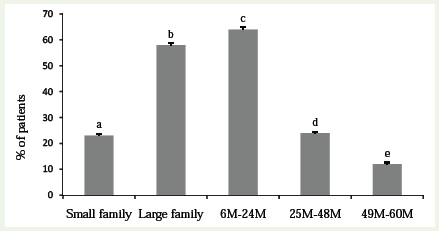
Figure 2: Distribution of PEM patients according to family status and age. Data are shown as mean ± SD for triplicate of each group. a-eSubscript letters shown on the bar graph indicate that the values are significantly different(Tukey multiple range, post hoc test, p< 0. 05) from each other (*p< 0.05, SPSS for windows, version 18.0).
Figure 3 described the weaning status of the PEM children. Immunization history of the patients revealed that 80 children (80%) were incompletely vaccinated while 9% were completely vaccinated and 11% children were nil vaccinated.
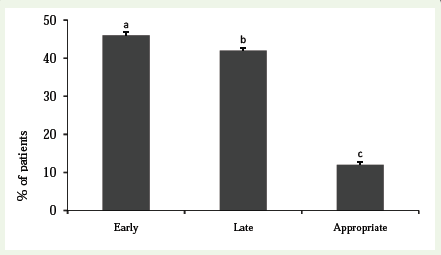
Figure 3: Distribution of patients according to time of weaning. Data are shown as mean ± SD for triplicate of each group. a-cSubscript letters shown on the bar graph indicate that the values are significantly different (Tukey multiple range, post hoc test, p< 0. 05) from each other (**p< 0.01, SPSS for windows, version 18.0).
In this studies (14%) PEM children had eye sign as with Bitot’s spot (2%) who had frequency 14.28%, 3% children had pus/ inflammation with frequency 21.42% and 7% children had corneal clouding with frequency 50.01% where corneal ulceration was observed in 2% children with frequency 14.29%. Almost all of (14%) them were deficient of vitamin D. Among the PEM children, 18% had mild dermatosis with frequency 28.12%, 29% had moderatedermatosis with frequency 45.12% where 17% children had severe dermatosis with frequency 26.56%. 39% of the studied patients had kwashiorkor, 25% had Marasmus-Kwashiorkor with massive oedema of both legs, while 36% patients had Marasmus.
In this observation 68% male and 32% female were admitted where 58% were rural and 42% urban living. The patient’s parents were illiterate 62%, primary 24%, secondary 12%, above 2%, who practices early weaning 46%, late weaning 42%, poor socio-economic population was at risk as with associated problem with tuberculosis7%, acute respiratory infection 25%, diarrhea 39%, Septicemia 29% in PEM.
Discussion
The study correlated the laboratory findings of PEM children from Chittagong with clinical presentations. As an exploratory investigation on serum electrolytes status severely malnourished children, having different socioeconomic background and living pattern. This study revealed some of important risk factors of PEM atChittagong region in Bangladesh. The risk factors and side effects of PEM are determined by different parameters such as, socioeconomic condition of both urban and rural areas in the patient attending at CMOSGH. Family history and anthropometrics variables like height, weight, age, sex, vaccination status, MUAC, pattern of feeding, timeof weaning, eye signs, types of dermatosis, types of malnutrition, serum electrolyte level for blood routine examination of TC, DC with neutrophil, lymphocyte, eosinophil, monocyte, and hemoglobin level were estimated.
Analysis of serum electrolyte in both the groups revealed that hypokalemia, hyponatremia and low serum bicarbonate were seen more frequently in patients who had diarrhea, as compared to patients who had not diarrhea. In a study performed at Agra by [14] estimation of electrolytes was done in 126 children with malnutrition where the cases were divided into four clinical groups:undernutrition, marasmus, nutritional oedema and kwashiorkor. Serum K+ levels ranged from 3.2 to 6 mmol/L. Serum K+ levels were low in 21.30% of non-oedematous children as contrasted to 33.3% of oedematous group. The overall mean values in non-oedematous and oedematous groups were 4.80 and 4.18 mmol/L respectively, which isapproximately similar to our study. As regards the nutritional status, most cases of electrolyte disturbance were seen in those who had diarrhea of variable duration. A similar type of study was conducted in Egypt by Said et al. [15] to find comparatively the electrolytes in plasma and electrolytes in PEM. Their study also revealed that plasma K+ is markedly lower than normal in all groups of malnourished subjects.
The results of the hyponatremic and hypokalemic studies were consistent with the other previous studies [16]. The results of this study showed significant association with previous studies in Bangladesh and worldwide. From this investigation we can say that our findings have similarity with previous studies. Prevention of malnutritionat a large scale can be accomplished through improvement in the socioeconomic status and coordinated as also well-planned efforts in the field of agriculture, education, social services and public health. Preventive action should be taken at the levels with family,community, national and worldwide.
In the study, we found that eye sign present in 14% patients, where edema present 64%, with frequency of 28.12% mild oedema. In the three socioeconomic classes of the studied subjects the prevalence was found in lower class 90%, Middle class 80%, and higher class 2%,because poor economic parents cannot give the child as they needed. We distribute patient according to pattern of feeding as artificial 02%, breast feeding 08% mixed 05%, and mal-feeding 85% because in Bangladesh people are as educated in 62.5% where our findings we find that 62% are illiterate, from 100 patients who do not know the food value and which food contain how much amount and givefood illiterally. That is, PEM patients are at risk as with associated problem. As our findings 7% children are suffer from tuberculosis, 25% patients from ARI, and had diarrhea 39%, also suffer 29% patients from septicemia and other side effects of PEM due to their food habit and life style. Since at CMOSGH the patients are mostlyurban, the percent distribution shown here may vary to some extent, also found higher prevalence of PEM in urban compare to rural. A prospective study was undertaken to study the clinical profile and pattern of infection in 90 Ethiopian children with severe PEM [17]. Study group consisted of 44 (49%) with marasmus, 29 (32%) withM. kwashiorkor and 17 (19%) with kwashiorkor. Their age ranged from 4 to 60 months and the median age at admission was 11.5, 15 and 20 months respectively. Over 80% patients were infected and lungs were the commonest sites. Bacterial pathogens predominantly gram negative enteric organisms were isolated from 36% of blood and37% of urine specimens tuberculosis and non-typhoidal Salmonellae showed a higher tendency of causing disseminated disease. Rickets and overt vitamin a deficiency were seen in 37% and 17% of thepatients respectively. Septicemia, gastroenteritis, pneumonia and disseminated TB accounted for an overall case fatality rate of 32% which support our study [17]. Good antenatal care so that mother’s own nutrition remains up to the mark and she does not develop malnutrition and anemia. This will be of much help in reducing theincidence of intrauterine growth retardation and low birth weight infants- the predecessor of malnourished children in very many instances. Encouragement to the mother’s to breastfeed the infants for as long as they can. Even if the mother’s not in a position to breastfeed the infant for some reason, it is of advantage to express her milk and feed to him. Of course, she must take good diet andadequate amounts of fluids to maintain her lactation.
[18] At the age of 6 months, the infant should start receiving nutritional supplements, in addition to breastfeeding. The supplements should be combination of cereals, protein-rich foods and fruits such as mashed banana. The practice of shifting to artificialfeeding in the form of bottle feeding with diluted cow milk or tinned milk should be discouraged, particularly in the poor in whose families it is virtually impossible to prevent occurrence of contamination of the bottle and the formula. Here again nutritional education is of vital importance. Its delivery may be either through mass media such as radio, television, posters, documentary, films etc, or imparting knowledge to the mothers at group meetings or at the doorstep of the family by the health auxiliary.
Secondly, surveys to detect cases of mild to moderate malnutrition, using preferably age independent criteria, should be conducted. Such children may be kept under surveillance and if required given nutritional supplements. The supplementary feeding programsin Bangladesh include applied nutrition program, midday meal program for school children. Especial nutritional program, vitamin A prophylaxis program, anemia prophylaxis program, integrated child development services (ICDS), food for work program, etc. The principal beneficiaries of such programs are the nutritionally vulnerable preschoolers, school-going children and pregnant andlactating mothers. Ample evidence is now available to support the contention that adequate supplementation through the feeding programs results in improvement of nutritional status of the target population, provided that operational efficiency is ensured. This consists of measures to improve food production, control price-risemake available cheap supplementary foods, fortify and enrich foods, prevent adulteration and irradiate certain foods such as wheat, potato and onion. Also, nutrition education and containment of population explosion are of paramount importance, various international foodprograms like those of WHO, FAO, UNICEF, CARE, OXFAM,SIDO, DANIDA, Indo-Dutch, etc.
Electrolytes changes were commonly seen in malnourishedpatients particularly who were presented with diarrheal episodes of variable duration. If this changes are diagnosed in time and treated appropriately the morbidity and mortality could be decreased. It was observed that the inflammatory response had increased in childrenwith PEM. [19] PEM children are potentially susceptible to high oxidative stress. It is concluded that electrolytes disturbances in malnourished children may be sub-clinical but become obvious during diarrheal illness. Measurement of serum electrolyte, therefore, is helpful for immediate therapy to avoid serious life threatening situation because most of the electrolyte disturbance were observedin those who had diarrhea of variable duration.
Conclusion
The results demonstrate that protein energy malnutrition significantly affects the electrolyte balance in children to cause diarrhea and worsen the diarrheal events. PEM children suffering from diarrhea also achieve more vulnerability to other secondary infections like acute respiratory infections, septicemia, tuberculosisetc. at least in monitored area of Bangladesh. Electrolyte measurement, monitoring and supplement can help the PEM children from serious life threatening situation.
References
- Mesham AR, Chatterjee M (1999) Wasting away: The crises of malnutrition in India. Washington DC. The World Bank, Washington, D.C.
- Mubarak A, Atta-Ullah M, Abid H (2003) Acute hypokalemic flaccid paralysis in malnourished children. Pak Pead J 27: 166.
- Afridi HI, Kazi TG, Kazi N, Kandhro GA, Baig JA, (2011) Evaluation of status of calcium, magnesium, potassium, and sodium levels in biological samples in children of different age groups with normal vision and night blindness. Clin Lab 57: 559-574.
- Adelman RD, Solhang MJ (2000) Pathophtysiology of body fluids and fluid therapy in Behrman RE, Kleigman RM, Jenson HB (eds) Nelson text book of Pediatric 16th ed. California WB Saunders, USA.
- Franco V, Hotta JK, Jorge SM, Dos Santos JE (1999) Plasma fatty acids in children with grade III protein-energy malnutrition in its different clinical forms: Marasmus, marasmic kwashiorkor, and kwashiorkor. J Tropical Ped 45: 71-75.
- Gupte S, Pal M (1987) Some issues in protein-energy malnutrition. Indian Pract 40:1037.
- Cervantes-RÃos E, Ortiz-Muñiz R, MartÃnez-Hernández AL, Cabrera-Rojo L, Graniel-Guerrero J, RodrÃguez-Cruz L (2011) Malnutrition and infection influence the peripheral blood reticulocyte micronuclei frequency in children. Mutat Res 731: 68-74.
- Bairagi R, chowdhury MK, Kim YJ, Curlin GT, Gray RH (1987) The association between malnutrition and diarrhea in rural Bangladesh. Int J Epidemiol 16:447-481.
- Jelliffe DB, Jelliffe EEP (1992) Causation of Kwashiorkor: Towards a multi-factorial consensus. Pediatrics 90: 502.
- Marghoob AA, Blum R, Nossa R, Busam KJ, Sachs D, et al (2001) Agminated atypical (dysplastic) nevi: case report and review of the literature. Arch Dermatol 137: 917-920.
- Gupte S (1998) The Short Textbook of Pediatrics. Nutritional deficiency state:8th ed., Japee Brothers Medical Publishers, Dehli.
- Bhutta ZA, Nizami SQ, Thbani S, Issani Z (1997) Risk factor for mortality among hospitalized children with persistant diarrhea in Pakistan. J Trop Paedtr 43: 330-336.
- Gupta MC, Manjusha M, Sunita A, Meenakshi S (1991) Human Nutrition Unit, All India Institute of Medical Sciences and Nutrition Research and TrainingCentre, Indian Council of Medical Research, New Delhi. Relation with childhood malnutrition of parental education and mothers nutritional related KAP. Ind J Paed 58: 269-274.
- Kalra V, Grover J, Ahuja GK, Rathi S, Khurana DS (1998) Vitamin E deficiency and associated neurological deficits in children with protein-energy malnutrition. J Trop Pediatr 44: 291-295.
- Abi-Said D, Annegers JF, Combos-Cantrell D, Suki R, Frankowski RF, et al. (1997) A case control evaluation of treatment efficacy:the example of magnesiums sulfate prophylaxis against eclampsia in patients with preeclampsia. J Clin Epidemilol 50: 419-423.
- Majeed R, Shamsi AH, Rajar U (2006) Clinical manifestation of hypokalemia. J Liaquat Univ Med Health Sci 2:50-53.
- Shimeles D, Lulseged S (1994) Clinical profile and pattern of infection in Ethiopian children with severe protein-energy malnutrition. East Afr Med J71: 264-267.
- Gopalan C (1993) Child care in India: Emerging challenges. Indian Pediatr 30:593.
- Aggarwal KN (1982) Grading of PEM in reference to Harward standard. Indian J Pediatr 49: 395-396.